Introduction
There are two types of transgastric feeding tubes used in children’s services at Addenbrooke’s Hospital. These are:


Your nurse specialists will meet you and show you the type of tube that your child will have and teach you how to care for it. This leaflet, which discusses both types of transgastric jejunal feeding tubes, contains information about tube insertion and tube care as a reference for you. The leaflet has five parts:
- Part 1: General information about what a jejunal feeding tube is, why it has been recommended for your child and the advantages and disadvantages related to jejunal feeding tubes.
- Part 2: Commonly asked questions
- Part 3: How to care for and use a PEG J tube
- Part 4: How to care for and use a MIC GJ tube
- Part 5: Contact details and details of your child’s tube
Part 1: General information
What is jejunal feeding?
Rather than delivering fluid and food into the stomach, jejunal feeding delivers fluid and nutrition directly into the jejunum.
What is the jejunum?
The small intestine is part of the gastrointestinal tract between the stomach and the large intestine (also known as the colon). The small intestine is where most of the water nutrients from food are absorbed.

The small intestine is divided into three parts:
- The duodenum
- The jejunum
- The ileum

What is a transgastric feeding tube?
Transgastric feeding tubes combine both a gastrostomy tube (which is placed in the stomach) and a jejunal tube (which is placed in the jejunum). The tube therefore has two access ports, one for the stomach and one for the jejunum. These are clearly labelled on the tube. By having a combined type of tube, the option of giving (where appropriate) fluids, feed or medicines into the stomach and/or the jejunum exists.
When a transgastric jejunal tube is inserted, the feeding tube enters in through the stomach. It then passes down through the muscle at the bottom of the stomach (called the pylorus), through the duodenum and into the jejunum.
Why has a transgastric jejunal feeding been recommended for my child?
There are a number of reasons why a child might have a transgastric jejunal tube and your doctor and nurse specialist will explain these to you.
Some of the common reasons are:
- Children who have had a recurrence of their gastro-oesophageal reflux after a Nissen’s fundoplication operation and for whom a ‘redo’ Nissen’s fundoplication is not likely to be in the child’s best interests/ helpful.
- Children who have severe gastro-oesophageal reflux but for whom a Nissen’s fundoplication may not be in their best interests.
- Children with gastric dysmotility problems.
- Children with acute pancreatitis.
- For children who cannot tolerate gastric feeding (i.e. feeding into the stomach).
- Children who have had major surgery on their gastrointestinal tract.
- Children with a high risk of aspiration (also known as aspiration pneumonia). Aspiration pneumonia happens when a liquid, such as fluids or food from the stomach, goes into the lungs.
Advantages of a transgastric jejunal feeding tube:
- Ensures the child receives their hydration and nutritional requirements when they are unable to do so by other means.
- Prevents the need for a nasojejunal tube which can be less cosmetically pleasing, is more likely to be accidentally pulled out and is difficult to insert.
- Allows for the stomach to be accessed so, if tolerated, some fluid, feed or medicine can still be administered into the stomach.
- Allows air to be removed from the stomach.
- Reduces the risk of aspiration.
Disadvantages of a transgastric jejunal feeding tube:
- Usually an operation is required to pass the tube the first time.
- An operation is usually needed to change/ remove a percutaneous endoscopic gastrostomy-jejunostomy (‘PEG J’) tube.
- The jejunal tube can migrate (go back) into the stomach and so need replacing.
- The child who requires jejunal feeding will have to be fed over many hours of the day and night. This is because, unlike the stomach, the jejunum is not a storage organ and so cannot tolerate ‘boluses’. Instead, feed must be slowly dripped into the jejunum. This is achieved through a pump being connected most of the time which can slowly administer the feed.
- The tube can be pulled out and will therefore need replacing.
- The tube can get blocked and will therefore need replacing.
- The tube can suffer from a mechanical failure and so need replacement.
Part 2: Commonly asked questions
Where will I get supplies of the consumable items from?
- Your gastrostomy care team will provide you with an initial seven to 14 day supply of equipment.
- In most areas an ongoing supply of equipment can be delivered to your home. Your care team will arrange this while you are still in hospital. If this service is not available in your area, your care team will ensure that alternative arrangements are in place for you.
- You should remember to order new supplies in good time before you run out and only use equipment for the length of time specified by the manufacturer.
Can I/my child bath and shower?
- Yes! Showers are permitted after 24 hours and baths after 48 hours.
- Always ensure that the tube end is closed and, where applicable, the clamp applied. Dry the area thoroughly afterwards.
Can I/my child go swimming?
- Yes! Ensure the tube end is closed and, where applicable, the clamp applied.
- If your child has a PEG J tube you may prefer to coil the tubing under a waterproof dressing.
- Although it is not clinically necessary to do so, some swimming centres request that the tube is covered. Check with your local pool.
Will I/my child be able to go to school?
- Your child should be able to go to school as normal.
- Staff at the school must be taught what to do if the tube falls out and spare supplies should be kept at the school for emergency use.
Can we go on holiday?
- It is fine to travel with your child but it is advised that you discuss travel plans with your doctor/ care team. It may be helpful, particularly if your child has complex needs, to take a letter with you from your doctor which can help you if you need to seek medical advice whilst on holiday. In addition letters from your care team can be useful to prevent any problems with airport security when you are travelling with ‘medical equipment.’
- Remember to take extra supplies with you and to pack at least some of these in your hand luggage in case your main luggage goes astray.
- Use a large dressing to avoid getting sand near the stoma site as this can irritate the skin.
- Your home delivery company may offer to give practical advice.
- We have a leaflet with advice titled “Going on holiday with a gastrostomy/ jejunostomy tube – advice for parents/carers “. Please ask for a copy if you could like one.
Part 3: How to care for and use a PEG J tube
What is a PEG J tube?

A PEG J tube (also called a percutaneous endoscopic gastro-jejunal tube) combines both a gastric and jejunal feeding tube. The following is a diagram of a ‘Fresenius’ PEG J tube:

How is a PEG J tube inserted?
- A PEG J tube is inserted under general anaesthetic.
- The first part of the procedure involves inserting the gastric part of the tube. To do this a gastroscope (a flexible instrument with inbuilt camera) is passed through your child’s mouth, down their oesophagus (food pipe) and into the stomach. The stomach is then filled with air and a needle is passed through the skin into the stomach. The tube itself is inserted by it being threaded down the oesophagus, into the stomach and out through the hole made by the needle.
The internal flange remains inside the stomach and an external fixation plate is applied next to the skin to hold the tubing in place. - Once the gastric part of the tube is in place the jejunal part of the tube is threaded down the inside of the gastric tube. This is watched on an x-ray machine to ensure that the jejunal tube is put into the correct position.
- (If your child already has a PEG gastrostomy tube of sufficient size, the jejunal tube can be threaded down through the existing gastrostomy tube.)
Caring for a PEG J tube
PEG J tube complications and ‘problem solving’
Complications regarding PEG J tubes include:
- displacement of the jejunal part
- mechanical failure
- overgranulation
- tube blockage
- discharge from the stoma site
- feed leakage from the stoma site
- infection
These complications can be managed as detailed below in the section titled ‘problem solving’.
Serious complications related to PEG J tubes are very rare and symptoms are seen usually within a maximum of 72 hours after insertion or change. If your child develops any of the ‘red flag’ symptoms within 72 hours of PEG J tube insertion or change you should contact the paediatric surgery nurse specialist team. The nurse specialist team is available Monday to Friday 08:00 (8am) to 18:00 (6pm) on 01223 586973 excluding bank holidays. Outside of these hours you should speak to your GP or local hospital who will contact the paediatric surgery specialist registrar at Addenbrooke’s.

The ‘red flag symptoms’ are:
- Pain on feeding OR
- Signs of distress on feeding OR
- Prolonged or severe pain post procedure OR
- Fresh bleeding OR
- External leakage of feed around the tubing
Problem solving
Jejunal tube displacement:
Although it is highly unlikely for the gastric part of the PEG J tube to come out, it is possible for the jejunal part to dislodge. This most commonly occurs when the child is being lifted or when the tubing gets caught on the wheel of a buggy/ wheelchair. Ensure care is taken to prevent accidental pulling that can lead to dislodgement.
It is possible to identify the position of the tip of the jejunal tube by aspirating a small amount of fluid and testing its level of acidity (called ‘pH’) on special paper. If the tip is in the correct position, the pH should be six to eight. If the tip has moved into the stomach the pH will be one to five. You may also be able to aspirate feed from the stomach where previously you had been unable to do so.
If you do not have any pH paper, it is possible to gain information about the position of the jejunal tube by performing a 'blackcurrant test'. Administer approximately 10ml of undiluted blackcurrant cordial via the jejunal port. After five minutes, aspirate via the gastric port. If blackcurrant is aspirated this is a strong indicator that the jejunal tube has migrated (moved) into the stomach.
If the jejunal tube has displaced or you suspect that it may have done so, apply the clamp, tape the tubing to your child’s skin to prevent any further dislodgement and call your nurse specialist/ community nurse. Your child will, in most cases, need to come to Addenbrooke’s Hospital where an x-ray may be taken to confirm the tube’s position and further intervention to resolve the problem may be required under general anaesthetic.
Mechanical failure of the PEG J tube:
Unfortunately, with repeated use, parts of the PEG J tube can fail. If the connectors fail (e.g. start to leak) or break, these can be replaced by the nurse specialist team in clinic or on the ward.
In some children, disconnection of the jejunal tubing from the connector has been observed. In these circumstances, if the jejunal tube can still be seen within the outer gastric tubing, the nurse specialist team may be able to repair the PEG J tube. In cases where the jejunal tubing has passed into the stomach, tube replacement will be required. If you suspect a disconnection has occurred, apply the clamp and do not use the tube at all; seek urgent medical attention.
Overgranulation and its management:
Granulation tissue is the result of the body trying to repair itself. You may recognise overgranulation as a clear brownish discharge and occasional bleeding or as pinkish raised tissue. If bleeding occurs or a large amount of tissue builds up, contact a member of your care team for advice as treatment may be required in the form of a dressing or ointment.
Tube blockage and its management:
To prevent tube blockage the tube should be flushed regularly and medications administered in a way that limits the chances of tube blockage occurring (see sections on ‘flushing’ and ‘administering medications’).
If the tube does block you may try the following. If unsuccessful in the first step, move onto the next:
- Ensure the clamps are released.
- Ensure the tube does not have any twists/ kinks.
- Massage the tube around the area of blockage if it is obviously visible.
- Try to flush with warm water using a ‘pumping action’ with the plunger on the syringe.
- Connect a 60 ml syringe to the end of the tube and try to draw back (’aspirate’).
- Mix half a teaspoon of sodium bicarbonate (baking soda) with 30ml of boiling water. Leave this to cool to a warm temperature then use a syringe to flush this solution down the tube. Leave the solution in the tube for two hours and then try to flush it through with warm water.
- Contact a member of your care team for advice.
Do not:
- Try to administer fruit juices/ fizzy drinks down the tube in an attempt to unblock it.
- Attempt to unblock the tube by inserting objects down it.
- Use excessive force.
If the tube is irreparably blocked it will require changing in theatre under a general anaesthetic.
Discharge from the stoma site and its management:
It is usual to experience a discharge from the stoma site until the stoma heals (usually 7 to 10 days after placement). It is important to clean the area carefully during this time.
If the discharge is spoiling clothing, a small medicated dressing (eg honey based dressing or anti-microbial dressing) can be applied but this should be changed regularly/ removed when no longer needed.
If discharge continues to be seen contact your community or specialist nurse as this may indicate gas bloat, pooling of gastric secretions or a poorly fitting fixation plate.
Feed leakage from the stoma site and related management:
If feed is observed coming from the stoma site you should contact your community nurse or nurse specialist as this may indicate that the jejunal tube is no longer in the correct position.
Managing the child with vomiting/diarrhoea:
- Always check expiry dates of the feed.
- Ensure the feed is brought up to room temperature before administering it. Feed straight from the fridge may be too cold.
- The rate (speed) of the feed may need to be reduced, contact your nurse specialist/ community nurse or dietitian.
- The speed at which medications are given may need to be reduced, contact your nurse specialist or community nurse.
Part 4: How to care for and use a MIC GJ tube (low profile balloon retained transgastric-jejunal feeding tube)
What is a low profile balloon retained transgastric-jejunal feeding tube (MIC GJ)?
A MIC GJ tube (also called a low profile balloon retained transgastric-jejunal feeding tube) combines both a gastric and jejunal feeding tube. The tube is held in place by an inflatable balloon which is situated inside the stomach (labelled externally as BAL on the tube) and a ‘low profile bolster’ which sits externally next to the skin. The external bolster contains two access ports, one for the stomach (labelled gastric) and one for the jejunum (labelled jejunal). Each access port has a one way valve within it. The valve is opened by attaching an extension set. Pictures of the MIC GJ tube and extension set are shown below:
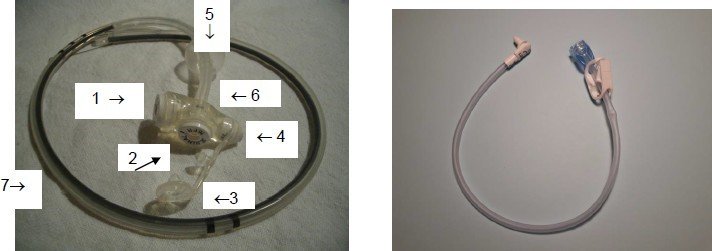
External part (i.e. visible at skin level)
1 = Gastric port (to side of device)
2 = Jejunal port (on top of device)
3 = Feeding port cover
4 = Balloon inflation port
Internal part (i.e. inside the child’s stomach/ jejunum)
5 = Retaining balloon
6 = Internal gastric part of the tube
7 = Internal jejunal part of the tube
How is a MIC GJ tube inserted?
If your child already has a low profile balloon retained gastrostomy tube, your child will usually be able to have the MIC GJ tube inserted in the interventional radiology x-ray department whilst your child is fully awake or after being given sedation.
In the interventional radiology department, the gastrostomy tube is removed and the MIC GJ tube is inserted through the same hole (‘stoma’). This is watched on a monitor to make sure that the jejunal part is correctly positioned.
If your child does not have a low profile balloon retained gastrostomy tube, your child will usually have the MIC GJ tube inserted in the operating theatre under general anaesthetic.
Your nurse specialist will explain which procedure is planned for your child and why.
Caring for your MIC GJ tube
Flushing:
- To prevent blocking, both the jejunal and gastric ports needs to be flushed regularly.
- The tubes should be flushed with cooled, boiled water.
- Flushes should take place before a continuous feed is started and when it is stopped. In addition, a flush should be given before and after a medicine is put down the tube. If more than one medicine is being given, a flush should also be given between each medicine (see section on administration of medicines).
- Your dietitian will specify the amount of water to be used to flush the tube.
- If the gastric access port is not being routinely used, flush every 24 hours with 10ml of water.
- If the jejunal access port is not being routinely used, flush every 6-12 hours with 5-10 ml of sterile water.
Using an extension set:

- It is not appropriate to insert a syringe directly into the device (as it can break the inner valve). Therefore, every time that the MIC GJ tube is accessed, whether this is to give medicines, feed, flushes or for decompression, an extension set must be used.
- A different extension set should be used to access the gastric port and the jejunal port.
- The extension sets should be changed once per week.
- To prevent complications with the feed valve it is important that the same brand of extension set is used as Mic GJ tube itself.
- Between each use the extension set used in the gastric port should be cleaned with hot soapy water and then left laying to dry on a clean, flat surface (if the child is under one year or is immune compromised the extension set should be sterilised).
- Between each use the extension set used in the jejunal port should be cleaned with hot, soapy water and then sterilised.
How to connect the extension set to the access port:
- Wash hands.
- Place a finger and thumb on either side of the bolster and open the feeding port cover (see diagram above).
- Line up the black mark on the extension set with the black mark on the access port.
- Push the extension set downwards into the access port.
- Rotate the extension set in the direction marked with the arrow (i.e. clockwise) until you feel resistance (this will be felt after a three quarter turn). This locks the extension set in place.
How to remove the extension set from the access port:
- Wash hands.
- Place a finger and thumb on either side of the bolster.
- Rotate the extension set in the direction opposite to that marked by the arrow (i.e. counter/anti clockwise) until the black mark on the extension set is in line with the black mark on the access port.
- Gently pull the extension set upwards and out of the access port.
- Cover the access port with the feeding port cover.
Administering fluid/ feed via a MIC GJ tube:
- It is important to always wash your hands carefully before and after using the tube.
- Your child’s dietitian will recommend a feeding plan suitable for your child’s needs.
- Because your child will need to have their feed delivered slowly over the course of many hours, it will be given via a feeding pump (machine). Your children’s nutrition nurse specialist will arrange teaching on how to use this pump. The pump will be fully portable for ease of use at home. Information leaflets about the actual pump itself will be provided for you.
- It is not necessary to check the position of the tube before starting the feed unless you are concerned that the tube does not have its normal appearance, for example looks like it may be falling out.
- Before the feed is started and when it finishes, water needs to be given to prevent the tube from blocking. This is normally at least 20 ml but your dietitian will advise you on the exact amount for your child. If the water is being given from a syringe, it must be pushed in very slowly (2 to 3 ml per minute). The water used should have been boiled and then allowed to cool.
Procedure:
- Wash hands.
- Set up the pump as shown by the children’s nutrition nurse specialist.
- Apply the clamp and then connect the extension set as described in section ‘How to connect the extension set’ above.
- Flush the tube with cooled boiled water with. . . . . . . ml of water (remember to unclamp the extension set).
- Connect the feed as shown by the children’s nutrition nurse specialist.
- Once the feed has been completed, wash your hands and flush the tube with . . . . . . . ml of water.
- Apply the clamp and then disconnect the extension set as described in the section ‘How to remove the extension set.’
Replacing feeding sets:
- Feeding sets need to be changed every 24 hours.
MIC GJ tube ‘problem solving’
Emergency action to take if the tube falls out:
It is possible for a MIC GJ tube to be pulled out if sufficient force is exerted on the tubing. It is therefore important to ensure that the tubing is not allowed to get caught, for example whilst lifting your child or while pushing your child in their buggy/ wheelchair.
A Mic GJ tube can also fall out if the internal balloon perishes (see section on ‘procedure for changing the water in the balloon’). If the tube does get pulled/ falls out, the gastrostomy stoma can close within one to two hours and therefore it is essential that immediate action is taken.
Your care team will organise for you to have a low profile balloon retained (‘gastrostomy button’) which you can insert in an emergency situation to prevent the tract from closing (you will be taught how to do this by your community nurses and/or nurse specialists).
Procedure:
- Take the button gastrostomy device from the emergency kit box
- Gently insert the button into the gastrostomy stoma
- Draw up 5ml of water into the syringe from the ampoule in the emergency kit box
- Inflate the retaining balloon
- You should then contact your nurse specialist who will arrange for your child to have a new Mic GJ tube inserted.
What is an emergency kit box?

You will be supplied, by your nurse specialist, with an ‘emergency kit box’ to keep your child’s emergency equipment (spare button device, extension set and syringes) in. It is essential that your child’s emergency kit box is carried with your child at all times including to school, hospital visits, trips out or on holidays.
Concern that the jejunal tubing has migrated back into the stomach
It is possible, with repeated retching or, due underlying dysmotility, for the jejunal part of the Mic GJ tube to migrate back up into the stomach from the jejunum. Symptoms of a migrated jejunal tube include:
- vomiting of feed
- aspiration of feed from the gastric port despite it being delivered via the jejunal port
- pain or discomfort on feeding
- being able to physically see the tip of the jejunal tube during a child’s vomit (see section below ‘tip of jejunal tube has been vomited up into the child’s mouth’)
It is possible to identify the position of the tip of the jejunal tube by aspirating a small amount of fluid and testing its level of acidity (called ‘pH’) on special paper. If the tip is in the correct position, the pH should be six to eight. If the tip has moved into the stomach the pH will be one to five. Some medications alter the pH so it is advised to take an aspirate from the child’s gastric port and one from their jejunal port simultaneously and compare the two results. If the pH is the same from both samples then the jejunal tubing has probably migrated back into the stomach.
If you do not have any pH paper, it is possible to gain information about the position of the jejunal tube by performing a 'blackcurrant test'. Administer approximately 10ml of undiluted blackcurrant cordial via the jejunal port. After five minutes, aspirate via the gastric port. If blackcurrant is aspirated this is a strong indicator that the jejunal tube has migrated (moved) into the stomach.
In any instance when you are concerned that your child’s jejunal tube may have migrated back into the stomach it is important to call your nurse specialist without delay so that urgent review can be arranged to (1) remove the MIC J tube to prevent complications such as coiling/ knotting in the stomach or vomiting of the jejunal tube up into the child’s mouth and (2) to replace the tube.
Tip of jejunal tube has been vomited up into the child’s mouth
If the jejunal tube on a MIC GJ tube has migrated back up into the stomach and this has not been recognised or, no action taken, it is possible (although extremely rare), for the child to then vomit up the tip of the jejunal tube so it is seen in the child’s mouth. Whilst it will be extremely distressing to observe such a situation, it is essential that you remain calm and take immediate action as the tubing will cause a choking response.
Action to take:
- Keep calm.
- Insert a luer slip (clear) syringe into the balloon valve on the MIC GJ device (marked ‘BAL’).
- Aspirate the syringe to remove all of the water from the retaining balloon.
- With a gentle but continuous action pull on the MIC GJ tube bolster (the part with the gastric and jejunal ports) until the entire length of tubing has been removed.
- To prevent the gastric stoma (hole) from closing now that there is no tubing in place, you will need to follow the directions in section ‘Emergency action to take if the tube falls out’).
- Contact your nurse specialist/ community nurse to arrange insertion of a new Mic GJ tube.
Balloon will not deflate:
If you cannot extract water from the balloon with the syringe:
- Ensure the syringe has been inserted correctly. If the syringe has been pushed in too far or not far enough, water will not be expelled from the balloon.
- Ensure the recess in the balloon valve is clean. Occasionally this recess can trap spills of feed or other material. Clean inside the recess with warm water (cotton buds are useful for this) then try to insert the syringe again by pushing it firmly into the valve with a push and twist motion.
- If the balloon will still not deflate you should contact your community nurse or nurse specialist.
Mechanical failure of the device
Unfortunately, with repeated use, parts of the Mic GJ tube can fail. If the connectors fail (e.g. start to leak) or break, these can often be temporarily taped in place until tube replacement can be arranged.
Tube blockage and its management:
To prevent tube blockage the tube should be flushed regularly and medications administered in a way that limits the chances of tube blockage occurring (see sections on ‘flushing’ and ‘administering medications’.
If the tube does block you may try the following. If unsuccessful in the first step, move onto the next:
- Ensure the clamps are released.
- Ensure the tube does not have any twists/ kinks.
- Try to flush with warm water using a ‘pumping action’ with the plunger on the syringe.
- Connect a 60ml syringe to the end of the tube and try to draw back (’aspirate’).
- Mix half a teaspoon of sodium bicarbonate (baking soda) with 30ml of boiling water. Leave this to cool to a warm temperature then use a syringe to flush this solution down the tube. Leave the solution in the tube for two hours and then try to flush it through with warm water.
- Contact a member of your care team for advice.
Do not:
- Try to administer fruit juices/ fizzy drinks down the tube in an attempt to unblock it.
- Attempt to unblock the tube by inserting objects down it.
- Use excessive force.
If the MIC GJ tube is irreparably blocked it will require changing. This may be in the x-ray department or in the operating theatre.
Overgranulation and its management:
Granulation tissue is the result of the body trying to repair itself. You may recognise overgranulation as a clear brownish discharge and occasional bleeding or as pinkish raised tissue. If bleeding occurs or a large amount of tissue builds up contact a member of your care team for advice as treatment may be required.
Discharge from the stoma site and its management:
It is usual to experience a discharge from the stoma site until the stoma heals (usually 7 to 10 days after placement). It is important to clean the area carefully during this time.
If the discharge is spoiling clothing, a small dressing can be applied but this should be changed regularly/ removed when no longer needed.
If discharge continues to be seen contact your community or specialist nurse as this may indicate gas bloat, pooling of gastric secretions or a poorly fitting fixation plate.
Feed leakage from the stoma site and related management:
If feed is observed coming from the stoma site you should contact your community nurse or nurse specialist as this may indicate that the jejunal tube is no longer in the correct position.
Leakage from the feed valve:
The feed valve is designed as a valve which closes each time the extension set is disconnected. This prevents stomach/ jejunal contents from coming out when the extension set is disconnected.
Using a syringe directly into the feed valve or a non-approved extension set (that is, one which is of a different brand to the Mic GJ tube itself) can break this valve. Ask your community nurse or nurse specialist if you have concerns relating to the feed valve.
Managing the child with a vomiting/ diarrhoea illness:
- Always check expiry dates of the feed.
- Ensure the feed is brought up to room temperature before administering it. Feed straight from the fridge may be too cold.
- The rate (speed) of the feed may need to be reduced, contact your nurse specialist/ community nurse or dietitian.
- The speed at which medications are given may need to be reduced, contact your nurse specialist or community nurse.
Part 5: Contact details
If you have any queries or need further information:
Your community nurse:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Your nurse specialist: 01223 586973
Details of your child’s tube:
Brand of transgastric jejunal tube:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Size:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Gauge:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Gastric length:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Jejunal length:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
Date of insertion:
. . . . . . . . . . . . . . . . . . . . . . . . . . . . .
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/