
Who is this information for and what is its aim?
This information sheet is for the parents of any child diagnosed with talipes / clubfoot and aims to further explain the boots and bar - the long term bracing stage of the Ponseti technique. This is the final stage of the Ponseti treatment and is central to the success of the management for clubfoot. It is therefore essential that this stage of treatment is fully adhered to ensure the best outcome for your child; this leaflet aims to explain the importance of this stage.
What does this stage of the Ponseti method involve?
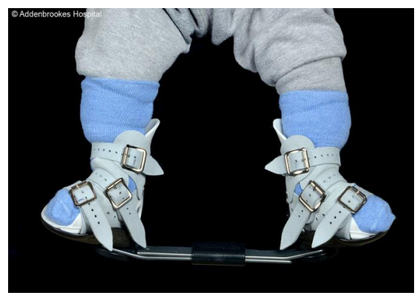
The final stage of the Ponseti method involves fitting your child with the boots and bar foot abduction brace after the final plaster cast has been removed. His / her feet and legs might look a little bit red, bruised and swollen, but this is normal and will settle down once the plaster has been off for a few days.
Babies can become upset when they are first put into the boots and bar, which can make it a little distressing for parents. This is because it is a new experience for them and frustrating to have both feet joined together by the bar and not usually because they are in pain. The feet can also be a little sensitive from the casting, and this takes time to settle. It is very important, however, to persevere with this challenging initial period.
We recognise that this can be a difficult time and the paediatric orthopaedic team are here to support you through this transition. We are here to provide advice about caring for your child in the boots and bar and to make any adjustments to the equipment in order to help your child settle into them.
Why are the boots and bar important?
The boots and bar hold the feet in the position needed to stop the muscles and ligaments becoming tight again and the foot position reverting to the original starting position.
Your child is at high risk of the clubfoot returning and further corrective surgery if the treatment prescribed is not strictly adhered to.
How long will the boots and bar need to be worn?
The boots and bar must be worn for 23 hours per day for the first three months. They can only be removed for a total maximum of one hour per day (e.g. at bath times), although this could be split into two lots of 30 minutes for example.
After three months, they are worn at night and nap time, for a minimum of 10 to 12 hours a day. During the day, your child can walk barefoot or wear well-fitting shoes. The boots and bar will need to be worn until your child is five years old.
The paediatric orthopaedic team will discuss with you if any changes to this routine are needed and will make the decision as to when the boots and bar are no longer needed.
Will my child need any other special equipment or clothing?
Your child can use a normal pram, car seat and high chair. Clothing with poppers or buttons between the legs can make it easier for dressing and undressing while the bar is in place.
Who fits the boots and bar?
A member of the paediatric orthopaedic team carries out the first fitting of the boots and bar. You will be shown how to fit them yourself, so that you can continue at home. Once the bar is set at the correct position for your child, this can only be altered by a member of the paediatric orthopaedic team.
How should the boots be fitted at home?
- The affected or most difficult foot is fitted with the first boot.
- Where both feet are affected, there is sometimes one foot which is less flexible than the other, this is the foot which should be fitted into the boot first, with the more flexible one fitted last.
- Your child should wear socks or tights at all times with the boots. Thin cotton socks are usually best as this helps to keep the boot as close to the foot as possible and should minimise rubbing. Sometimes socks with rubber gips on the bottom can also help, but again, these should be as thin as possible as thick socks can affect the fit of the boot. Socks should be changed on a daily basis.
- Make sure that your child’s heel is at the back of the boot and firmly down at the base of the boot
- Place the tongue over your child’s foot and secure the middle strap first. This needs to be done up as tightly as possible to prevent the foot from slipping which can cause problems with the skin and could lead to the foot tightening up.
- Once the middle strap is done up securely, the other straps can be done up.
- The other boot can then be fitted in the same way.
- Once the boots are securely on, the bar can then be fitted and clipped into place.
- Always check after fitting that the heels of both feet are down at the back of the boots. This can be done by looking at the hole at the back of the boot where you should see the heel down in the boot. If the heel has ridden up out of sight, the boots need to be removed and refitted to ensure the correct fit.
N.B when the boots are fitted for the first time in clinic, the heel may sit a little high in the boot for the first few days, but should lower into the boot with time; your clinician will discuss this with you when they fit the boots. - The position of the heels should be checked periodically through the day and reapplied if the position has changed. Wearing the boots with the heels too high carries the risk of rubbing and developing blisters.
How can I encourage my child to accept the boots and bar?
You can help your child accept the boots and bar by introducing playful exercises that teach your child to bend both knees at the same time. We will suggest some that seem to work. The more time that your child spends wearing the boots, the sooner she / he will get used to moving both legs together.
If you notice that your child is crying more than usual, please check that the boots are fitted correctly and also check for rubbing or blisters. If you find any blisters, please contact the team as soon as possible. Blisters can mean the boots are getting too small or that the bar needs to be widened.
Who adjusts the boots and bar?
The boots are set to a specific angle on the bar, which must not be altered by anyone other than a member of the paediatric orthopaedic team. They will do this at your regular check up appointments.
It can be useful to mark with a pen how tight the straps need to be initially, but do bear in mind that straps will loosen with use and so you may need to adjust the tightness of the straps accordingly. Again, your paediatric orthopaedic clinician will advise you on this.
How often will my child need to attend clinic?
The first clinic review will be one-two weeks after the first fitting of the boots and bar to ensure there are no problems in the initial stages.
The next clinic visit will be three-four weeks after this (half way through full time wear), followed by a third visit, six weeks later (at the end of full time wear).
Following reduction to night time wear, your child will be seen in clinic six weeks after this. All future follow-up appointments will be every three to six months.
When to contact the hospital
It is important to contact the hospital if you:
- Have difficulty in fitting the boots and / or bar yourself
- Are concerned that your child’s skin looks sore
- Think the boots and bar are becoming too small or are damaged
- Are concerned about any other aspect of your child’s feet
It is important to follow all of the above instructions carefully to ensure the treatment is successful. Staff involved in your child’s care will always be happy to answer any queries you have.
Remember: your child is at high risk of the clubfoot returning and further corrective surgery if the treatment prescribed is not strictly adhered to.
Useful contacts
- The paediatric orthopaedic team secretary: 01223 216101
- Email the paediatric orthopaedic physiotherapists
- The paediatric orthopaedic specialist nurse: 01223 254996 or 01223 245151 (bleep 159126)
- The plaster room: 01223 217772
- STEPS: The National Association for Children with Lower Limb Abnormalities (opens in a new tab)
- Ponseti group (International) (opens in a new tab)
If you have any problems outside normal working hours, please take your child to your local emergency department and contact one of the Addenbrooke’s team as soon as possible on the next working day.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/