Omnipod Handbook (Open Loop)
This booklet has been written to provide you, your family and/or carers, with the information you need when using an Omnipod DASH/ Omnipod 5 insulin pump.
Please refer to the additional closed loop supplement if using the Omnipod 5 with continuous glucose monitoring (CGM) in SmartAdjust.
Non-urgent advice: Insulet contact number
Telephone: 0800 011 6132 or +44 20 3887 1709 if calling from abroad
Please note that the pump companies will not give medical advice and can only offer technical support if you are having problems with the pump.
Website: Omnipod
Immediate action required: Urgent Advice
- If you are feeling ill or have an emergency diabetes or pump problem out of hours, contact the Type 1 Emergency Out-of-Hours Service.
- Contact the diabetes educators if you do not have this number
- Or attend your nearest accident and emergency department
Pump software for sharing data
Please set up a Glooko Personal account via the website.
Join Glooko (opens in a new tab)
You will need to link your Glooko account to our clinic using the ProConnect code: ukaddhos
Linking your Glooko account to our clinic
1. Log into your Glooko account at my.glooko.com (opens in a new tab)
2. Select “Settings” from the drop-down menu (top right on the home screen)
3. Scroll down to Account and select “+ Add New Code”
4. Select “Continue”
5. Enter ProConnect Code (ukaddhos) then select “Submit.”
If you have an Omnipod 5 pump, this will need to be linked to Glooko before data can come through.
1. Log into your online Omnipod account at www.omnipod.com (opens in a new tab), using your Omnipod ID
2. Go to the My Account tab and then select Account linking from the drop down menu. Then click “Link”
3. Select “sign up” or “log in” with Glooko
4. Proceed to Glooko and complete the process to link your account. When complete, your status will update to “Linked” and data will automatically upload into your personal Glooko account.
Non-urgent advice: Important Information
Insulin pumps provide clever technology to better manage glucose levels, but the basics remain important. These include:
- Accurate carbohydrate counting
- Entering all carbohydrates eaten into the pump (except hypo treatment)
- Timing of the mealtime/snack insulin – a bolus given 10-15 minutes before eating is recommended
- Regular pod changes
- Rotation of infusion sites
- Optimal hypo treatment
- Adjustments for activity
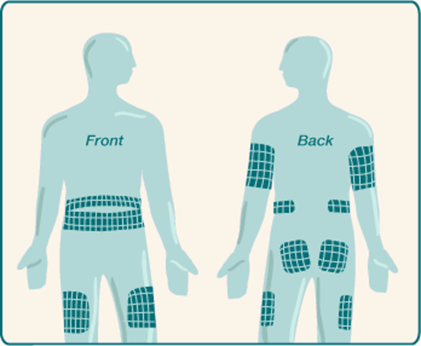
Changing the cannula sites (pod change)
Remember to rotate your injection sites
Your Omnipod pump should be changed every 72 hours or when the Pod's insulin reservoir is low or empty.
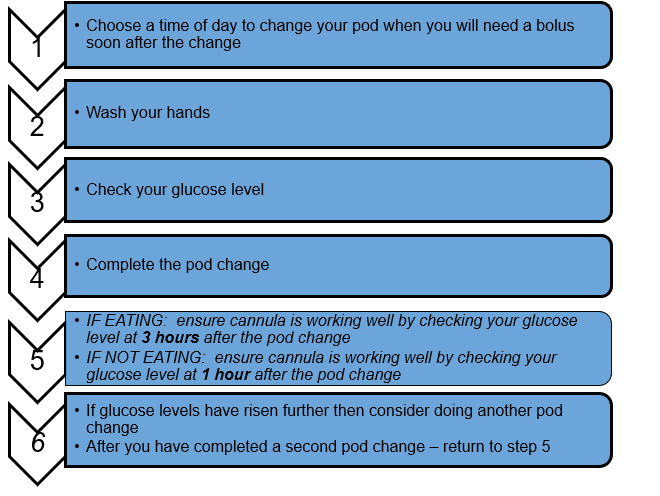
Ideally it is recommended that the pod change is completed before breakfast or lunch as this provides an opportunity to check the pod is working and effectively delivering insulin. The concern about changing the pod in the evening is that it could fail and you may not be aware of this problem overnight.
Below are some guidelines to ensure your pod changes run ‘smoothly’.
Painful cannula?
When doing a pod change, the new cannula might temporarily be uncomfortable, but it shouldn’t hurt for more than a few minutes. If it does, it might not be in the right spot, and it’s worth giving a small bolus (with something containing carbohydrate to eat!). If it still hurts, or hurts even more, then change the cannula straight away.
Cannula not sticking?
Before applying a new pod, clean and dry your skin well. Avoid getting body lotion, creams or oils near the site, as these products may loosen the adhesive. If you find that the tape on the pod still doesn’t stick well, consider spraying the area with an anti-perspirant first, allow the site to dry, ensuring it doesn’t leave a powdery residue, then insert the cannula. It is also a good idea to avoid very hairy areas or consider shaving the skin to allow the tape to stick firmly. If you find the pods tend to fall out when you become sweaty during exercise you may find something like the ‘Skin-Tac’ adhesive wipe or Cavilon barrier cream useful. These can be found online and some GPs may prescribe it. If possible, avoid taking a bath, shower or swim and getting the pod wet for at least two hours after applying it. There are options for tape, as well as ‘patches’ that stick over devices for an extra layer of protection or adhesion. Speak to the pump team for further advice if needed.
Insertion site irritation / redness?
If you experience redness/itchiness at the infusion site there are a number of things to consider;
- Be gentle in peeling back and removing your pod. You can try a ‘Lift plus’ or ‘TacAway’ spray/wipe, baby oil or olive oil to help if needed.
- Ensure you rotate where you place your pods. The adhesive will often remove several layers of skin when removed and will need time to rest and heal.
- If your skin becomes red and itchy underneath the sticky tape try applying some tea tree oil or a small amount of topical steroid cream onto the site once the cannula is removed. If the redness and itchiness persist, contact the Pump Team for advice.
- If there is pain, pus, warmth, or spreading redness that persists for 1-2 days after your pod is removed, please contact your GP for advice. You may have an infection and need antibiotics to treat it.
Please remember that rotating infusion sites is really important to prevent lipohypertrophy (lumpy sites) and allow good insulin absorption.
Non-urgent advice: Recommendations for checking your basal rates:
Recommendations for checking your basal rates:
- We would suggest starting with your overnight basal rates
- We would suggest doing these checks a few times on days that are similar to ensure there is a pattern before you make any changes
- Ideally your glucose level at the start of each check should be between 5 and 10 mmol/L (up to 12 mmol/L can work)
- Choose a day to basal check when you;
- Have not had a hypo of 3.5 mmol/L or below in the past 12 hours
- Have not been significantly more active than normal
- Have not been unwell or are under more stress than usual
- Have not had a significant amount of alcohol in the past 12-24 hours
- Abandon this check if you have a hypo or if your glucose levels go above 12 mmol/L and correct
| Time Frame | What to do | When to check glucose if not wearing a sensor |
|---|---|---|
|
Time Frame
Overnight check |
What to do
Begin review if pre bed glucose is 5-10 mmol/L Eat an evening meal that contains 50g or less carbohydrate that you are confident you will count accurately Do not consume any food or carb- containing drinks for the rest of the evening. Do not exercise |
When to check glucose if not wearing a sensor
3-4 hours after evening meal Bedtime (if not the same time as above) 2-3am On waking |
|
Time Frame
Morning check |
What to do
Begin review if pre-breakfast glucose is between 5-10 mmol/L Skip breakfast Eat no food until lunch |
When to check glucose if not wearing a sensor On waking and every 2 hours until lunch |
|
Time Frame
Afternoon check |
What to do
Begin review if pre-lunch glucose is 5-10 mmol/L Eat a breakfast that contains 50g or less carbohydrate that you are confident you will count accurately Skip lunch No food or carb containing drinks until evening meal |
When to check glucose if not wearing a sensor
3-4 hours after breakfast Then every 2 hours until evening meal |
|
Time Frame
Evening check |
What to do
Begin review if pre-dinner glucose is 5-10 mmol/L Eat a lunch that contains 50g or less carbohydrate that you are confident you will count accurately Do not have an evening meal or carb-containing drinks Eat a late snack if needed |
When to check glucose if not wearing a sensor
3-4 hours after lunch Every 2 hours until your late snack |
Non-urgent advice: Glucose levels
If the glucose levels rise or fall more than 2 mmol/L during the review period this can suggest the basal rates need adjustment.
Adjust the basal rate for the time period 60 – 120 minutes before and up to when the rise or fall in glucose occurs
Adjust the basal rate by 10-20% or by 0.05 or 0.10 units/hr either up or down depending on whether your glucose rose or fell
Bolus insulin and carbohydrate counting
All carbohydrates consumed should be covered with an insulin bolus unless you are treating a hypo or being more active. The amount of insulin required is calculated by your pump when you enter the carbohydrate in grams into the bolus calculator. If you choose to miss a meal or eat a meal that doesn’t contain carbohydrate you do not need to give a bolus of insulin unless your glucose level is raised at the time of the meal.
You may find that if you have several snacks and insulin boluses in a row, the insulin can build up in the body and work more strongly than intended, leading to a low reading later. This is called insulin stacking. If you notice that this is a pattern, please speak to your pump educator.
It is important to count your carbohydrates as accurately as possible. You may find the Carbs and Cals book/app (by Chris Cheyette) useful with carbohydrate counting – see the images shown below. We also offer regular Carbohydrate Counting Workshops. Please ask your pump educator to add your name to the waiting list if you feel this would be helpful.


Normal/Standard
The full amount of insulin is delivered immediately to cover the carbohydrates eaten. Most people start with this delivery until their basal rates and bolus ratios are correct.
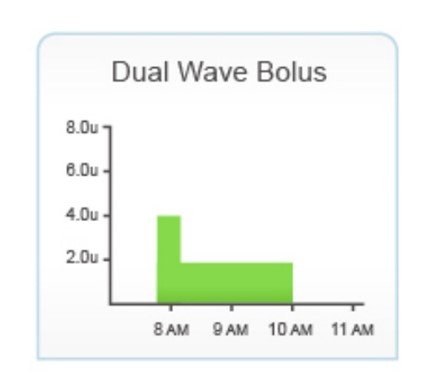
Extended Bolus
The insulin is delivered in 2 separate doses. The first bolus is delivered as a normal bolus before you eat and the rest is given over an extended length of time (30 minutes to 8 hours) as a square wave e.g. 50% given as normal and 50% given as square wave over 2 or more hours. This gives a better insulin match for larger meals containing a high amount of carbohydrate, protein and fat for example takeaways, pizza and curry.
| Timing | Target post meal glucose |
|---|---|
| Timing 2 hour post meal glucose | Target post meal glucose Within 2.8 mmol/L of pre-meal glucose |
| Timing 4 hour post meal glucose | Target post meal glucose Within 1.7 mmol/L of pre-meal glucose |
If the glucose level is out of target, review your insulin to carbohydrate ratio:
- If the glucose level rises higher than these levels increase the insulin dose by decreasing the carbohydrate ratio by 10-20% or by 0.5 to 1g
- If the glucose levels drop after a meal then reduce the insulin given by increasing the carbohydrate ratio by 10-20% or 0.5 to 1g
If at any stage during the process your glucose level drops below 4 mmol/L, abandon and have a snack. Repeat the process at another time to confirm the result.
Examples of how to change your ratio following a bolus check…
- Current insulin : carbohydrate ratio = 1unit:15g
Pre-meal glucose = 5.5 mmol/L, 2 hours post meal = 10 mmol/L
Increase the amount of bolus insulin by reducing the carbohydrate part of the ratio by 10-20% to 1unit:14g or 1unit:13g
Repeat the process to check whether the change was appropriate.
- Current insulin : carbohydrate ratio = 1unit:8g
Pre-meal glucose = 6.3 mmol/L, 2 hours post meal = 4.1 mmol/L
Reduce the amount of bolus insulin given by increasing the carbohydrate part of the ratio by 10-20% to 1unit:9g or 1unit:10g
Repeat the process to check whether the change was appropriate.
Note: The lower the carbohydrate ratio, the more insulin the pump will deliver to cover carbs. The higher the carbohydrate ratio the less insulin the pump will deliver to cover carbs.
| Possible cause | Possible solution |
|---|---|
|
Incorrect basal rate |
Possible solution
Check time on handset is correct If you use different basal patterns check you are using the correct one. Too much basal insulin for the activity and a reduced temporary rate basal is needed. Consider checking your basal rate if you notice there is a pattern of when your hypos occur. |
|
Incorrect bolus given |
Possible solution
Check bolus history Check that your carbohydrate counting is accurate Check the timing of bolus for food Consider type of bolus used |
|
Increased activity |
Possible solution
Consider a reduced temporary basal rate for future activity Consider extra carbs for future activity |
|
Hot weather |
Possible solution
Consider a different basal pattern for holidays or summer. Consider a reduced temporary basal rate. |
|
Drinking alcohol |
Possible solution
Consider a temporary basal overnight (up to 10am) if drinking more than 2 units or Consider a carbohydrate bedtime snack Consider reduced bolus at breakfast the next morning. |
|
Incorrect insulin |
Possible solution
Always check the following on a new insulin vial: insulin type, strength, expiry date and how it has been stored. |
It is important to share this information on correct hypo treatment with close family and friends so that they can assist you, if necessary, to treat a hypo safely.
- Remember to carry quick acting carbohydrate with you at all times for treating hypoglycaemia.
- Please contact your pump educator if you are having frequent, unexplained hypoglycaemia (more than 2-3 per week) or have an episode of severe hypoglycaemia.
How to manage glucose levels which are below target but not hypo
Pre meal/snack
When you enter a glucose level below target before eating your pump will deduct some insulin from the meal bolus to allow your glucose level to rise back into the target range. You may choose to give the bolus at the start rather than 10 minutes before.
If it is a large meal or high in fat it will take longer to digest so you may wish to split the bolus and deliver half at the start of the meal and the remaining half halfway through the meal.
In between meals
Have a small carbohydrate snack to raise your glucose to an appropriate level without covering with insulin.
For example 5g of carbohydrates will raise your glucose level by 1-2 mmol/L, 10g by 2-3 mmol/L.
Hypoglycaemia treatment flow chart
Glucose Level 3.5mmol/L or below (confirmed with fingerstick check)
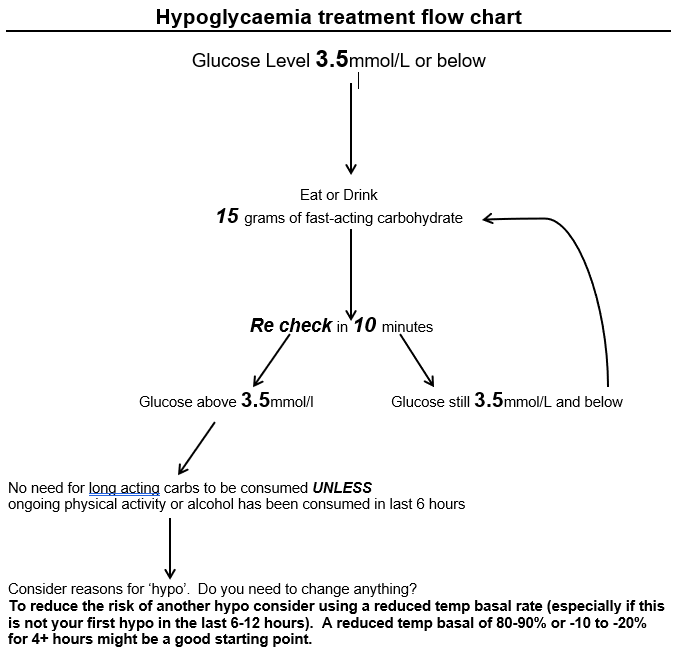
It is recommended not to correct a high glucose within 6 hours following a hypo and you may have to manually override your bolus dose to achieve this
Severe Hypoglycaemia

Severe hypoglycaemia is classified as a hypo requiring someone else to help you treat the low glucose level, meaning you would not have been able to treat it on your own.
Examples include:
- A family member recognising your hypo when you have missed it and helping you to treat it
- An unconscious hypo requiring a GlugaGen® injection
GlucaGen® Kit
It is very important that you have a GlucaGen® Kit at home and that someone in your household knows how to administer the injection. You can ask a healthcare professional to demonstrate how the kit is used. These kits will last until their stated expiry date if stored in the fridge and for 18 months if stored out of the fridge. Please remember to mark the date on the kit when you have removed this from the fridge if you decide to keep it out of the fridge.
We also suggest you carry a GlucaGen® Kit when you travel.
If a GlugaGen® injection has been administered:
- It can take 10-15 minutes to regain consciousness
- It is very important that once you are able to do so, you consume 20g of rapid acting carbohydrate e.g. 200ml pure fruit juice or 200ml normal cola and follow this with 40g slower acting carbohydrates e.g. 2 slices of bread or 4 digestive biscuits. This additional carbohydrate must not be covered with insulin.
- It is worth noting you may feel or be sick after the GlucaGen® injection. If this happens, then you will need to ensure you have the amount of carbohydrate listed above again. If you feel unable to eat, you can have carbohydrate in a drink form instead which you can sip slowly.
If no-one in your household feels comfortable using the GlucaGen® kit, or is worried you are taking too long to regain consciousness, they should call an ambulance.
It is very important that you make your diabetes team aware of any severe hypos that occur once commencing insulin pump therapy.
Urgent advice: Severe hypos
Please call the diabetes out of hours (Mon-Fri 4pm to 11pm and 6am to 9am, weekends and bank holidays 6am to 11pm) emergency number if you (or your relative/carer) require support during or following a severe hypo.
Speak with the diabetes team if you do not have this number.
| Possible cause | Possible solution |
|---|---|
| Possible cause Incorrect basal rate |
Possible solution
Check that the time on handset is correct If you use different basal patterns are you using the right one? Consider basal rate review |
| Possible cause Incorrect bolus given |
Possible solution
Check bolus history Check carbohydrate counting accuracy Check timing of bolus for food |
| Possible cause Less active/ more stress/ currently unwell/ menstrual cycle |
Possible solution
Consider using an increased temporary basal rate if the cause is temporary. |
| Possible cause Cold weather/high altitude/dehydration |
Possible solution
Consider a different basal pattern for holidays or winter Consider an increased temporary basal rate if the cause is temporary. Ensure that you drink enough. |
| Possible cause Insulin |
Possible solution
Always check a new insulin vial for damage, the use-by date, strength, correct insulin type. How long has your insulin been out of the fridge? Especially if the weather is hot. |
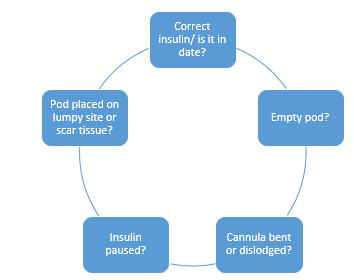
| Possible cause Blocked cannula/ faulty pod |
Possible solution
Are you due a pod change? Did your glucose levels rise with a recent pod placement? Is the infusion site wet? |
Symptoms of hyperglycaemia
- Thirst and dry mouth
- Nausea
- Urgency to urinate frequently
- Vomiting
- Frequent urination especially at night
- Dry or flushed skin
- Impaired vision
- Poor appetite
- Abdominal pains
- Muscular pains
- Difficulty breathing
- Apathy
- Odorous breath
- Fatigue, weakness
Troubleshooting the pump
If you are concerned that your PDM/ Omnipod 5 Controller may not be working, please call Omnipod’s Customer Care line immediately on 0800 011 6132.
Reduce the risks of hyperglycaemia by:
- Checking glucose levels 4-6 times daily (additional checks will be needed when unwell or exercising or pregnant)
- Using a correction bolus pre meals and pre bed as needed
- Changing your pod every 2-3 days
- Checking the cannula site regularly
- Checking insulin expiry date and use within 28 days if kept at room temperature. Be aware hot temperatures can cause insulin to degrade faster
- Accurate carbohydrate counting
- Using the bolus calculator
If you have forgotten your meal bolus and remembered 2 hours later because your glucose levels are high we recommend you take a correction dose rather than cover the carbs
Sick day rules and diabetic ketoacidosis (DKA)
A sudden onset of high glucose levels could become life threatening if not treated quickly. There are two common causes of rapid onset hyperglycaemia / DKA.
- Pump/ pod failure
- Illness
Monitoring your glucose levels frequently allows you to detect any significant changes in your glucose and therefore respond quickly.
When you are unwell, it is likely that your glucose levels will run higher because you become insulin resistant (caused by stress hormones) and need more insulin than normal. This response may occur even before you notice that you are unwell.
Insufficient insulin means the body cannot use glucose for energy and so fat is used as an alternative source. This breakdown of fat produces ketones and if the body cannot dispose of these ketones quickly enough they can build up in the blood to a harmful level. This is known as diabetic ketoacidosis (DKA) and if left untreated, can progress to coma or even death.
People using an insulin pump are more at risk of DKA in the event of a pod failure or failed cannula, because a pump uses quick acting insulin which is only active for 4 hours.
Actions to treat DKA
- Take extra insulin (see sick day rules flowchart on the next page)
- Drink plenty of sugar-free fluid (100-200mls water per hour)
- Do extra monitoring of glucose and ketones including overnight.
- Treat and seek help for the cause of your illness.
When unwell or you have 2 consecutive glucose readings above 14 mmol/L, always check for ketones and if present they should NEVER be ignored!
Things to have to hand at all times to prevent Diabetic Ketoacidosis (DKA)
- Quick acting insulin pen (in date)
- Blood glucose meter + strips (in date)
- Blood ketone meter + strips (in date)
- Extra pods (in date)
The following guidelines below will help you to work out how much more insulin you will need.
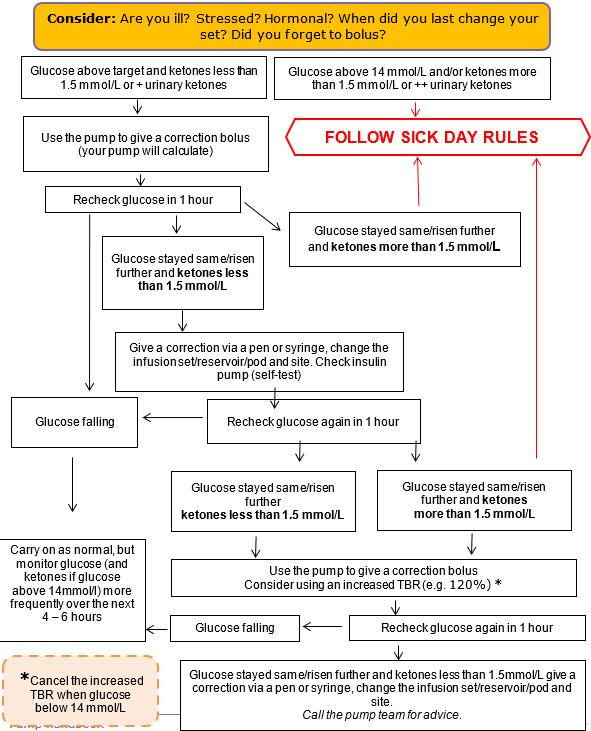
Sick day rules flowchart
Glucose higher than 13 mmol/L / you are unwell / blood ketones greater than 1.5 mmol/L or urinary ketones++
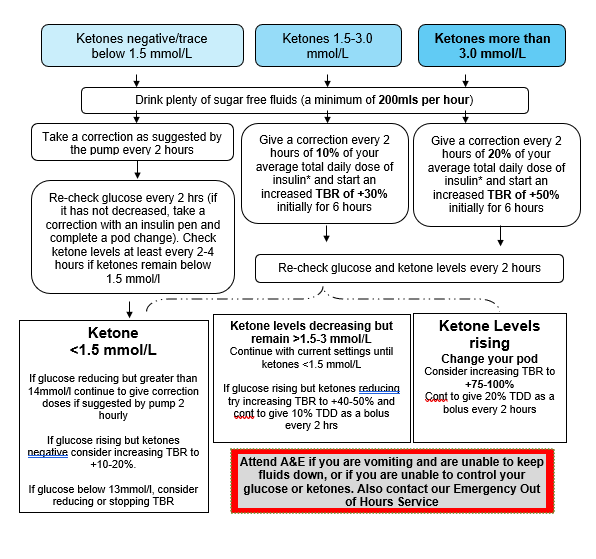
Ensure your Omnipod is working properly. If you have any doubts, change the pod and give a quick-acting insulin correction using a quick- acting insulin pen
*How to work out 10% and 20% of your Total Daily Dose (TDD) of Insulin
- Look up what your TDD is – this includes all your basal, bolus and corrective insulin in 24hrs.
- If you have an Omnipod 5, your TDD can be found on your Omnipod 5 Controller. Start by pressing the 3 lines in the top left of your Omnipod 5 controller. Then select ‘History Detail’. Then look at ‘Total Insulin’ (your TDD).
- If you have an Omnipod DASH, go to the Main Menu, select ‘History’, then ‘Insulin and BG History’ then navigate to the previous day. ‘Total Insulin’ is displayed in the bottom left circle.
- Alternatively you can get this information from your pump upload on Glooko.
- A quick way to work out what 10% of your TDD is to move the decimal point once to the left…
e.g. if TDD = 34 units then 10% = 3.4 units
- A quick way to work out what 20% of your TDD is to move the decimal point once to the left and times it by 2…
e.g. if TDD = 34 units then 10% = 3.4units x 2 = 6.8 units
- Or refer to the table below as an easy guide.
| Total Daily Dose | 10% (additional units) | 20% (additional units) |
|---|---|---|
| Total Daily Dose 20 | 10% (additional units) 2 | 20% (additional units) 4 |
| Total Daily Dose 30 | 10% (additional units) 3 | 20% (additional units) 6 |
| Total Daily Dose 40 | 10% (additional units) 4 | 20% (additional units) 8 |
| Total Daily Dose 50 | 10% (additional units) 5 | 20% (additional units) 10 |
| Total Daily Dose 60 | 10% (additional units) 6 | 20% (additional units) 12 |
| Total Daily Dose 70 | 10% (additional units) 7 | 20% (additional units) 14 |
| Total Daily Dose 80 | 10% (additional units) 8 | 20% (additional units) 16 |
| Total Daily Dose 90 | 10% (additional units) 9 | 20% (additional units) 18 |
| Total Daily Dose 100 | 10% (additional units) 10 | 20% (additional units) 20 |
Your diet when following sick day rules
If you cannot eat normally, try a light diet and eat smaller amounts more frequently e.g. every 2-3 hours. Examples include:
- Bread or toast with soup/egg
- Breakfast cereal
- Crackers/crisp breads/plain biscuits
- Milky puddings or yoghurt
- Milk or fruit juice
This can be supplemented with carbohydrate containing fluids such as milky drinks and fruit juices. Aim to consume a minimum of 30g carbohydrate every 6-8 hours. Cover this carbohydrate with your normal insulin bolus.
If a light diet is not tolerated, take sugary drinks in small amounts more frequently e.g. 10-15g carbohydrate taken every 1-2 hours, for example:
- Normal fizzy drinks (flat – may be tolerated better)
- Sugar-containing drinks e.g. pure fruit juice, cordial, milk
- Lucozade Original
- Ordinary jelly
Medicines
Tablet medications often contain very small amounts of lactose but will not significantly affect glucose levels (usually <2g of lactose per day). Most liquid medications are available in a sugar-free form but some liquids may contain significant amounts of sugar.
A single dose of a sugar containing medication is unlikely to significantly impact glucose levels. Discuss the availability of sugar-free medicines (including over-the-counter medication) with your pharmacist.
| Fast release carbs( shorter sessions/events | Carbs (g) | Slower release carbs (longer sessions/day events | Carbs (g) |
|---|---|---|---|
| Fast release carbs( shorter sessions/events Jelly Babies (4 sweets) | Carbs (g) 20 | Slower release carbs (longer sessions/day events Raisins (30g) | Carbs (g) 22 |
| Fast release carbs( shorter sessions/events Dextrose (4 sweets) | Carbs (g) 12 | Slower release carbs (longer sessions/day events Jaffa cake (each) | Carbs (g) 10 |
| Fast release carbs( shorter sessions/events Isotonic gel (each) | Carbs (g) 22-25 | Slower release carbs (longer sessions/day events Fruit bar (each) | Carbs (g) 15 |
| Fast release carbs( shorter sessions/events Energy sports bar (each) | Carbs (g) 25 | Slower release carbs (longer sessions/day events Cereal bar (each) | Carbs (g) 22 |
| Fast release carbs( shorter sessions/events Energy powder drink (500mls) | Carbs (g) 45-50 | Slower release carbs (longer sessions/day events Malt loaf (1 slice) | Carbs (g) 20 |
| Fast release carbs( shorter sessions/events Gatorade (250ml) | Carbs (g) 15 | Slower release carbs (longer sessions/day events Banana (medium) | Carbs (g) 15-20 |
| Fast release carbs( shorter sessions/events Lucozade Original (100mls) | Carbs (g) 8.4 | Slower release carbs (longer sessions/day events Flapjack (50g) | Carbs (g) 30 |
| Fast release carbs( shorter sessions/events Lucozade Sport (100mls) | Carbs (g) 6.4 | Slower release carbs (longer sessions/day events Fig roll (each) | Carbs (g) 14 |
| Fast release carbs( shorter sessions/events Cola (150ml - mini can) | Carbs (g) 15 | Slower release carbs (longer sessions/day events Oat cake (each) | Carbs (g) 6 |
| Fast release carbs( shorter sessions/events Apple Juice (120mls) | Carbs (g) 15 | Slower release carbs (longer sessions/day events Bread roll (50g) | Carbs (g) 25 |
Taking the pump off
There may be times when you would like to remove your Omnipod temporarily such as swimming, sex and going on holiday.
Insulin pumps should not be disconnected for more than 1–2 hours unless you follow advice in the table below. An Omnipod pump cannot be reapplied if you remove it. You will need to fill and place a new pod.
| Time off the pump for: | What to do: |
|---|---|
|
Time off the pump for:
Up to 90 minutes |
What to do:
Check glucose levels before removing the pod and give a correction if needed using the Omnipod handset. If eating use an insulin pen to give a quick acting insulin bolus to cover carbohydrates. When you place the new pod, check your glucose and give a correction if necessary. |
|
Time off the pump for:
Up to 4 hours |
What to do:
Check glucose before removing pod and give a correction if needed using the handset. At 2 hours after removing the pod use your insulin pen to give a bolus of quick acting insulin equivalent to the amount of basal insulin you have missed. For example if your basal rate is 1 unit/hour give a bolus of 2 units. If eating use an insulin pen to give a quick acting insulin bolus to cover carbohydrates. When you apply a new pod, check your glucose level and give a correction if necessary. |
|
Time off the pump for:
Up to 12 hours |
What to do:
Check glucose before removing the pod and give a correction if needed using the Omnipod handset. If eating use an insulin pen to give a quick acting insulin bolus to cover carbohydrates. Followed by either of the below: Every 2 hours use your insulin pen to give quick acting insulin equal to the missed basal amount or Take a dose of intermediate-acting insulin (Levemir or Humulin I) at the point of removing the pod that is equal to your basal insulin dose for the next 12 hours. If you choose to place a new pod before the 12 hours is up, please run a reduced temporary basal of ↓100% for the remainder of time. Finally: When you place a new pod, check your glucose and give a correction if necessary. |
|
Time off the pump for:
24 hours or longer |
What to do:
Check glucose before removing your pod and give a correction if needed using the pump. If eating use an insulin pen to give a quick acting insulin bolus to cover carbohydrates. Followed by one of the below: Every 2 hours use your insulin pen to give quick acting insulin equal to the missed basal insulin amount. or Take a dose of intermediate-acting insulin (Levemir or Humulin I) at the point of removing the pod that is equal to your basal insulin dose for the next 12 hours. You will need to do this injection twice, approximately 12 hours apart. If you choose to apply a new pod before the 12 hours please run a reduced temporary basal of ↓100% for the remainder of time. or Take a dose of long-acting insulin (Lantus) at the point of removing pod that is equal to your basal insulin dose for the next 24 hours. o If you choose to apply a new pod before the 24 hours please run a reduced temporary basal of ↓100% for the remainder of time. Finally: When you apply a new pod, check your glucose and give a correction if necessary via your Omnipod handset. |
| Time off the pump for: | What to do: |
Please note:
- If you remove your Omnipod for more than 4 hours, close monitoring of glucose levels is recommended.
- We would recommend that you discuss any plans to remove your pod with the pump team beforehand and plan ahead where possible. Disconnecting yourself from the Omnipod puts you at a higher risk of developing high glucose levels and forming ketones /DKA.
Travel

You may find the following link on the Omnipod website helpful to provide tips for managing travel:
Traveling with Diabetes | Omnipod UK (opens in a new tab)
Ahead of travelling contact the pump team for a travel letter to support you carrying your insulin pump supplies, sharps and liquids through security. The pump team will arrange this letter free of charge. Please contact us, if possible, 2 weeks prior to your departure.
Omnipod Pods, PDMs and Controllers can safely pass through airport x-ray machines. Pods are safe to be worn through airport scanners.
It is advised to keep all of your diabetes supplies with you in the cabin, not in the hold as it could freeze, which will damage them.
The Bluetooth® setting remains enabled in the Omnipod PDM/Controller’s aeroplane mode so they can communicate with your Pod.
If you are travelling to a hot/very cold climate or will be staying at altitude contact your pump team for support as you are likely to need adjustments to your settings.
Remember to change the time on your PDM when you reach your destination as well as when you return to the UK. For very long haul travel e.g. to Australia, it may be worthwhile making small changes to the time every 6 hours. The Omnipod 5 Controller will change according to time zones automatically.
Travel can be very stressful and therefore you may need to run an increased temporary basal to ensure your glucose levels are stable. Check glucose levels frequently and correct where necessary. Also remember to drink plenty of fluid.
Extra supplies for travelling
It is recommended that you take twice the amount of supplies (see above re supplies to carry if more than 1 hour from home) that you think you will use. Trips can be extended for reasons beyond your control.
Where possible divide your supplies with someone who is travelling with you or across two bags in case of theft or loss.
You will also need to carry quick acting and background insulin with you for emergency use if the pump fails. Please call Insulet in the event of your handset not working as they may be able to courier a replacement to you depending on where you are in the world.
It may be worth contacting your pump manufacturer (Insulet) well in advance to see if they have spare loan pumps for holidays in case of handset failure.
Insulet contact number Telephone: 0800 011 6132 or +44 20 3887 1709 if calling from abroad.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/