Introduction
Patients who have had a diagnosis of Heart Failure confirmed by a Cardiologist and have been referred to the Heart Failure Specialist Nurse team will be given this booklet.
The aim of this booklet is to provide information regarding your diagnosis, and also to advise you how to recognise and manage symptoms related to Heart Failure.
Who we are
We are the Addenbrookes Integrated Nurse-Led Heart Failure Team.
We are a team of Specialist Cardiology Nurses, who help people diagnosed with Heart Failure to manage their symptoms and to stay well.
We are an Integrated Team, which means we help patients admitted with symptoms of Heart Failure, as well as supporting people living with this condition at home.
We work closely with our Cardiology Consultant colleagues, who provide advice or support when required.
We have an Administration Team to support our work, who help book your appointments.
Please be aware that we are only able to support patients who are referred to our service. The referral to our service is via GP, General Cardiology and other specialist services.
What the service provides
The Heart Failure Service provides support in several ways. This support is available face-to-face, via telephone and also online.
After each consultation with the Heart Failure Specialist Nurse, we will ensure your GP is kept informed of any changes we have made to your management.
We are a specialist service, which means that we provide support while it is required. Once your symptoms are stable, our routine input will end, however your GP can refer you back to our service if our support is required again.
We offer support in the following ways:
Education - to help you understand your condition.
Support and advice - to help you when symptoms have increased.
Medication reviews - to ensure you are on the correct medication, and to provide the best outcomes for you.
Referral to other specialist teams. - These include Cardiac Rehabilitation, Breathlessness Intervention Service or Palliative Care (If required).
Links to Consultant Cardiologist Colleagues - We have regular meetings with our consultant colleagues.
Why you are attending this clinic
If you are attending our Clinic, you have been referred either by your GP or these other services.
Whilst you are in hospital - You were admitted to hospital due to symptoms of Heart Failure. While in hospital your diagnosis was confirmed by a Cardiologist. Or you may already be known to a Cardiologist.
Following GP Review - Your GP referred you to our service due to a suspected diagnosis of Heart Failure, or worsening symptoms of known Heart Failure. This referral was accepted, and you were seen in Clinic by a Cardiologist who confirmed your diagnosis and referred you to our Clinic.
Following Cardiology Review or Other Specialist Services - Your diagnosis of Heart Failure was confirmed, and this was explained to you in Consultant Clinic.
Heart failure specialist nurse-led clinics
There are a range of clinics available. (Education / Ambulatory Care/ Medication Optimisation). We will refer you to the correct clinic. You may be switched between clinics if this is required.
Education - Guides you through the initial stages of diagnosis, supporting you to manage your condition independently. These clinics are available as Face to Face or telephone consultations, or online.
Ambulatory Care - Allows closer monitoring and can help prevent prevents potential admission to hospital if symptoms become problematic. Attendance can be up to 3 times per week. We are able to adjust oral medications and can administer intravenous diuretics (medicine to reduce fluid levels in the body) and can refer you for Intravenous Iron infusions if these are required.
Medication Optimisation Clinic - For patients with reduced Left Ventricular function (HFrEF) only. These clinics allow adjustments to your medications to ensure you are on the best available combination. You will be seen in Clinic, at 1-2 weekly intervals, until your medication is optimised.
Brief Intervention Calls - Our Helpline is available to all patients on our caseload. These calls respond to voicemail messages left for our service. The voicemail is checked 3 times per day, Monday-Friday.
Normal Heart Function
The heart is a pump made from muscle.
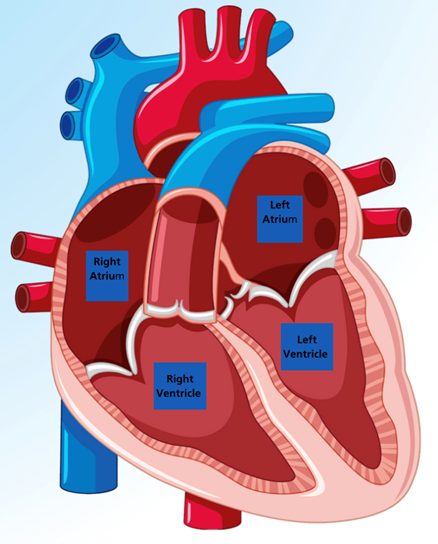
The heart is made from a special type of muscle that never gets tired in the way that other muscles do.
The heart pumps blood around the body via blood vessels.
Arteries (red) carry blood away from the heart to feed the body with oxygen and nutrients.
Veins (blue) carry blood back to the lungs to be refilled with Oxygen.
The direction of blood flow in the heart is controlled by valves, which open to let blood through and close tightly to prevent blood going back the wrong way.
The heart has 4 chambers. The 2 large chambers at the bottom are called ventricles and are the main pumping chambers of the heart.
The 2 smaller chambers at the top are called atria and receive the blood from the blood vessels when the heart relaxes between pumps.
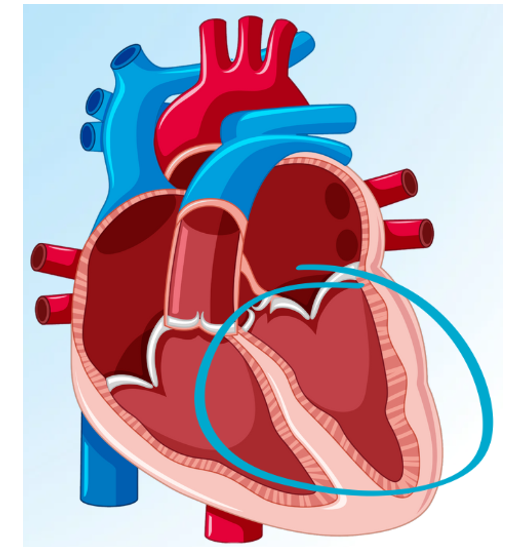
Left ventricular function
The pumping function of the ventricle is measured during the Echocardiogram.
Measurements of the blood in the chamber are taken before and after the heart pumps.
In a normal heart, at least 50% of the blood in the left ventricle is pumped out. If the force of the beat is weaker, less blood is pumped out. This is known as Left Ventricular Failure.
HErEF - Ejection Fraction less than 40% (Reduced Left Ventricular Function)
FHmEF - Ejection Fraction 40-49% (Moderately Reduced Left Ventricular Function)
HFpEF - Ejection Fraction 50% or more (Preserved Reduced Left Ventricular Function)
HFimpEF - Ejection Fraction, which has improved by at least 10% (Recovered Left Ventricular Function)
Your diagnosis will be explained to you by your Cardiologist. They will also explain which classification of Heart Failure you have.
This helps to ensure that you get the right treatment to manage symptoms and help you stay well.
Classifications of heart failure (HFrEF, HFmEF, HFpEF or HFrecEF)
Heart Failure with Reduced Ejection Fraction (HFrEF)
Less than 40% of blood is pumped out of the Left Ventricle with each beat.
These 4 main groups of medications have been recommended to improve heart function, manage symptoms and help you live longer. You may hear these medications referred to as the FOUR PILLARS. These medications are in the diagram below:

To get the greatest benefit for you, we will try and get these medications started for you as soon as possible. We have a Nurse-Led Clinic where we can manage this promptly for you to gain the biggest benefit.
Heart Failure with Mildly Reduced Ejection Fraction (HFmEF)
More than 40% but less than 50% of blood is pumped out of the Left Ventricle with each heartbeat.
Current guidance also recommends these medications, to improve symptoms and help you live longer. This also includes the ‘4 Pillar’ medications.
Heart Failure with Recovered Ejection Fraction (HFrecEF)
Also known as HFimpEF. (Heart Failure with Improved LV Function).
This is a new classification used by Cardiologists:
If the original Ejection Fraction is less than 40% and improves by more than 10% , this is known as Improved Ejection Fraction.
This improvement depends on the medications you are taking, so please don’t stop taking them unless the Cardiologist asks you to.
Taking your medication and following the lifestyle advice we provide is a key part of your recovery and continued stability.
Heart Failure with Preserved Ejection Fraction (HFpEF)
More than 50% of blood is pumped out of the Left Ventricle with each heartbeat.
The heart function issue is due other reasons than the function of the left ventricle. These could be:
- Thickening of the heart muscle wall. This makes the heart cavity smaller.
- The heart wall becomes stiff and can no longer relax between beats. This leads to less blood being pumped on the next beat.
- Problems with the heart valves. Valves can either become narrowed (Stenosis) or leaky (Regurgitation).
Medications for HFpEF are used to manage the symptoms. Medication currently available to help you stay well are SGLT2-Is and MRAs.
Managing symptoms
The main symptoms associated with Heart Failure are Fatigue, Breathlessness and Swollen legs.
When the heart is unable to pump out as much blood as it used to, it causes a build-up of blood in the body. This is called Congestion.
Fatigue
When the heart is unable to pump properly, oxygen and nutrients are unable to get to the muscles. This leads to tiredness.
Oedema or Swelling
When the heart is unable to pump properly, blood tends to pool in the blood vessels. The extra pressure from this fluid causes the blood vessels to leak into the surrounding tissues.
If the fluid leaks into the tissues of the lungs, it can cause increased breathlessness or phlegm production. You may also notice a new productive cough. A productive cough is when you expectorate mucous or phlegm.

If the fluid leaks into the tissues of the legs or abdomen, it causes swelling known as Dependent Oedema.
Regardless of where the fluid is stored, there will be an increase in body weight.
Breathlessness, wheezing or coughing
Buildup of fluid in the lungs takes up space where air would normally go. This leads to breathlessness, particularly when doing activities such as walking or climbing stairs.
Some people find they have trouble lying flat in bed and use extra pillows to help them breathe comfortably.
Breathing exercises can help too. They allow you to practise filling your lungs completely and making full use of your chest muscles.
Symptom monitoring and the NYHA scale
The New York Heart Association Functional Classification (NYHA) is an easy way for doctors and nurses to measure how much symptoms are affecting your ability to perform day to day activities.
By using the NYHA scale yourself, you may be able to notice how well you are doing, or to notice when symptoms are increasing.
This will hopefully help you notice symptoms early and guide you to seeking advice and assistance.
NYHA 1 I can perform all ordinary physical activities without getting overly short of breath or experiencing tiredness or palpitations.
NYHA 2 I have slight limitation of physical activity. I get shortness of breath, tiredness or palpitations when performing more strenuous activity such as walking up a hill or climbing several flights of stairs. I remain comfortable at rest.
NYHA 3 I have noticeable limitation of physical activity. I get shortness of breath, tiredness or palpitations when performing activities less trenuous than ordinary activity. I remain comfortable at rest.
NYHA 4 I am unable to carry out any physical activity without discomfort. I feel tired and short of breath even at rest. If any physical activity is
undertaken, discomfort from my symptoms is increased.
| Date | Weight | Date | Weight | Date | Weight |
|---|---|---|---|---|---|
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
| Date | Weight | Date | Weight | Date | Weight |
Vital signs
We recommend that you check your blood pressure and heart rate regularly.
If you can, please consider buying blood a pressure monitor to use at home. You can buy one for £20-£30 either online or from your local Pharmacy.
Alternatively, most GP surgeries and health centres have B/P measurement equipment. Pharmacies also offer B/P monitoring.
A blood pressure machine usually provides a heart rate but will not detect irregularities in your heart rhythm. It is much more accurate to take the pulse yourself.
Pulse oximeter machines are available online. Alternatively, you can find your own pulse and count how many times you feel it in one minute.
If your pulse feels irregular, it could be a sign of an irregular rhythm.
The most common irregular rhythm is Atrial Fibrillation (AF). This rhythm is more common over the age of 65.
If this rhythm is new, you should let your GP know.
How to take a pulse

It is important to measure a resting heart rate, so sit and relax for 5 minutes before measuring.
Hold out your non-dominant hand with your palm facing upwards.
Press your index finger and middle finger of your other hand on the side of your wrist, just below the base of your thumb. Don’t use your thumb as it has its own pulse.
Press the skin lightly until you feel the pulse - if you can’t find it press a little more firmly or move the fingers slightly.
Once you find your pulse, count the beats you feel for 60 seconds.
A normal heart rate is between 60 and 100 beats per minute. If your heart rate is continuously above 120bpm or below 40bpm, we recommend you make an appointment to discuss this with your GP.
| Date | B/P | Pule | Date | B/P | Pule |
|---|---|---|---|---|---|
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
| Date | B/P | Pule | Date | B/P | Pule |
Medicine therapies for heart failure

Symptom control medication - managing symptoms associated with fluid build-up in the body. These symptoms are listed next to the amber heart:
- Furosemide
- Bumetanide
- Metolazone


Prognostic Medication
ACE Inhibitors (....pril)
ARBs (....sartan)
ARNIs (Entresto)
MRA (Spironolactone/Eplerenone)
Beta-Blockers (...olol)
SGLT2-1 (...flozin)
Intravenous Iron
Cardiac Rehabilitation
Most of the medications to help you stay well and manage symptoms work through the kidneys. Kidney function is always monitored closely when making changes.
Medications for heart failure
Some medications can make you feel worse before you feel better. If you feel you are struggling to take your medications for any reason, please call the Helpline or your GP to discuss this rather than stopping them yourself.
These medications help your heart to pump more effectively and some even treat the underlying cause of the Heart Failure.
Managing your medications could help improve breathing and energy levels, increase your activity levels and improve fluid levels.
These medications can also help your heart to function better and help keep your symptoms stable.
These medications have been proved to help improve your quality of life, and to experience fewer symptoms. This will be discussed with you in Education Clinic in more detail.
Side effects
Severe reactions may occur with Intravenous Iron I nfusion preparations, although they are rare. They usually occur within the first few minutes of administration.
Please let your infusion nurse know if you feel any unusual symptoms when the infusion has been started.
There are common milder side effects listed, such as nausea, rash and injection site reactions.
Please report these to your infusion nurse if you notice any.
Delayed reactions may also occur and can be severe. These include aching in the bones or muscles and sometimes fever. The onset varies from several hours up to four days after the infusion. Symptoms usually last two to four days and settle on their own or following the use of simple analgesics.
How to stay well

Make Us Aware
Please call us on our Helpline when you start noticing an increase in symptoms. If we are aware, we can help.
Manage
Heart Failure is a chronic condition that can be managed. Following these recommendations can help symptoms to stay stable.
- Take Care with how much fluid you drink. Advice will be given in Clinic on what amount to try and aim for. If you are drinking more than 2 Litres (4 pints) of fluid per day, you are likely to be advised to reduce this. Milk with cereal or soup is not counted in your fluid intake.
- Alcohol - Please try not to drink more than 14 units alcohol per week, as this can be harmful to your heart. If you need help, please speak with us or with your GP.
- If you are a smoker, it is of vital importance that you stop smoking. Support is available, please ask if you need support with this.
- Eat a healthy, balanced diet. If you are overweight, you will feel better if you lose weight. Advice on healthy eating is available if you require advice.
- If we advise you to reduce your salt intake, as salt can make you hold onto fluids. Cooking with salt is fine but try not to season at the table. Please do not use Salt substitutes such as Lo-Salt as this contains Potassium. Please also try and avoid salty drinks such as Bovril or OXO. Also try and cook with reduced salt stock cubes or herbs and spices. Ready meals are often high in salt, so try and avoid these if possible.
- Exercise is of vital importance and has a huge effect on staying stable. Exercise will not harm you and can be increased safely. Exercise can even make you feel better by making you fitter overall. Always make sure to pace yourself and try not to rush. Cardiac rehabilitation is an excellent service to help increase exercise levels safely. Your HFSN or your GP will be happy to refer you if you would like to participate.
- Please ensure you have any immunisations you are offered, to protect you from potentially serious illnesses.
- Anxiety is common if you have heart problems. If you feel anxious, taking slow deep breaths can sometimes help. If anxiety is impacting you daily life, we can signpost you to services that can help you. Alternatively, please speak with your GP.
Monitor
- Please remember to weigh yourself every day.
- If you can, please keep a record of your heart rate, blood pressure and weight so you can quickly spot any changes.
- Please keep a record of your medications.
Make Us Aware
- Please report any changes to symptoms, even if you are not feeling unwell.
- Please report any issues you may have with medications.
- Please report any changes you think may be due to your condition.
Heart failure or cardiology resources
Pumping Marvellous (opens in a new tab) (opens in a new tab) or 01772 796542
British Heart Foundation (opens in a new tab) (opens in a new tab)
British Society for Heart Failure (opens in a new tab) (opens in a new tab)
The Breathlessness Intervention Service or 01223 349325
Heart Failure Matters (opens in a new tab) (opens in a new tab)
Medication Resources
Dapagliflozin (opens in a new tab) (opens in a new tab)
Sacubitril/Valsartan (Entresto) (opens in a new tab) (opens in a new tab)
Other Heart Failure Medications (opens in a new tab) (opens in a new tab)
Older Adults Resources
Age UK (opens in a new tab) (opens in a new tab)
Cambridgeshire County Council (opens in a new tab) (opens in a new tab)
Non-Cardiology Resources
Psychological Wellbeing Service (IAPT) (opens in a new tab) (opens in a new tab) or 0300 300 0055
Hospice UK (opens in a new tab) (opens in a new tab) /Information and Support (opens in a new tab) (opens in a new tab)
Sue Ryder palliative, neurological and bereavement support (opens in a new tab) (opens in a new tab)
Arthur Rank Hospice (opens in a new tab) (opens in a new tab) or 01223 675777
MyChart
We would encourage you to sign up for MyChart. This is the electronic patient portal at Cambridge University Hospitals that enables patients to securely access parts of their health record held within the hospital’s electronic patient record system (Epic). It is available via your home computer or mobile device
More information is available on our website: MyChart
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/