Introduction
This leaflet provides information for parents and families whose baby has been diagnosed with gastroschisis. It aims to support the discussion you have had with your baby’s consultant and team.
What is gastroschisis?
Gastroschisis is a rare condition (affecting approximately one in every 4000 births) in which the baby’s abdominal wall does not form completely whilst the baby is in the womb. Early in all pregnancies, the intestine develops inside the umbilical cord and then, at about 10 weeks of pregnancy, usually moves inside the baby’s abdomen. In gastroschisis the intestine develops outside the baby’s body, through a hole, usually to the right of the belly button. There is also no protective covering (membrane) over the intestine, so when the baby is born, the intestine is open to the air. Gastroschisis is usually detected on ultrasound scans performed during pregnancy. If not detected prenatally (before birth) it is immediately apparent at birth.
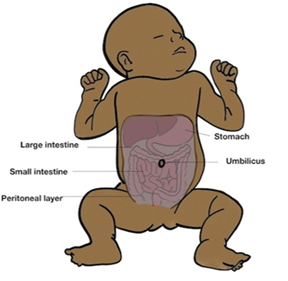
The diagram below shows the normal position of the organs in a baby’s abdomen:
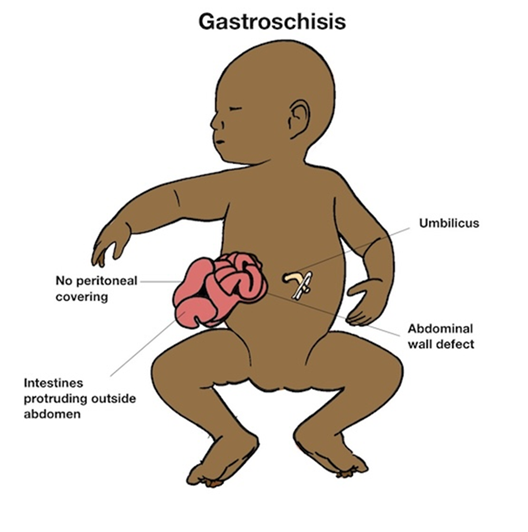
The diagram below shows the appearance of gastroschisis with abdominal content protruding (herniating) outside the abdominal wall:
What causes gastroschisis?
We do not know what causes gastroschisis. During pregnancy your baby will be monitored to check the condition of the bowel, to look for any signs of dilatation (widening) within the bowel and to check your baby’s growth. If there are any signs of concern, there is an increased risk of your baby being born prematurely and an earlier delivery of your baby may need to be arranged.
Signs and symptoms
Babies born with gastroschisis have some of their intestines outside their body when they are born. We must protect this bowel as soon as the baby is born with a covering such as cling film to prevent the baby losing fluid.
What happens after birth?
A team of neonatal doctors and nurses will be present at the birth of your baby. If your baby is well at birth you will be able to have a quick cuddle. Your baby’s bowel will initially be protected with a covering such as cling film. This reduces the amount of fluid and body heat lost, protects the intestine from further damage and also allows staff to monitor closely. A tube called a nasogastric tube will be inserted, via your baby’s nose and into their stomach, to help decompress the bowel. Lines will be inserted into veins to give fluids, nutrition and medication including antibiotics.
The children’s surgical team will review your baby and assess the condition of the bowel including its colour, looking for any signs of unhealthy or irreversibly damaged bowel (necrosis) and looking for any tears or holes in the bowel (perforation).
We will transfer your baby to our Neonatal Intensive Care Unit (NICU) to provide close monitoring.
Treatment and Management
Once stable, your baby will need an operation under general anaesthesia. The operation performed will depend on how much intestine is on the outside and on the condition of the bowel. In some cases, the defect can be closed at the first operation (a primary closure) but in other cases a staged repair is needed, replacing the intestine a part at a time. Sometimes a ready-made mesh, called a silo, is placed over the intestines so that they are contained and can gradually move back into the abdomen over approximately a week, prior to closing the muscle defect in the abdominal wall.
What happens after the operation?
Breastfeeding is encouraged as it has particular benefits for babies who have problems with their intestines. Breastmilk is often much better tolerated than formula, and even if you don't intend to breastfeed in the long-run it is worth considering expressing breastmilk for the first weeks. Even though the baby may not be able to have feeds in the first few days we can use colostrum for mouth care, which is a positive experience for the baby and boosts their immune system. It is important to start expressing as soon as possible after delivery and the midwives can help with this.
Being apart from your baby will be difficult and we will show you how to have positive touch experiences from the start even if a cuddle might not be possible right away.
Length of hospital stay
We know from a UK national research study that a third of babies born with gastroschisis are discharged within a month of life, a third take up to two months and a further third (usually those with more complex problems) will have a more prolonged hospital stay.
Long term outlook and ongoing problems
Babies born with gastroschisis usually have good outcomes. However, 5-10% of babies are considered 'complex' and show one of four complications: bowel perforation, bowel necrosis, bowel atresia (a blockage in the bowel where a segment of intestine is closed off or missing) or bowel not functioning properly (referred to as short gut). Complex cases may need additional surgery and prolonged line feeds.
More information about the Neonatal Unit
Parents are allowed to visit at all times, but there is limited accommodation available for parents of babies on the Neonatal Unit. We try to provide accommodation around the time of admission, surgery and in preparation for discharge home. If you would like to visit the Rosie neonatal unit prior to delivery, please ask the foetal medicine team to contact the Neonatal Intensive Care Unit (NICU) to arrange this. A short video introducing the NICU is also available in the Neonatal Services section of the Rosie Hospital website .
Support for you and your child with gastroschisis
- Contact a Family is a UK-wide charity (opens in a new tab) providing advice, information and support to the parents of all disabled children - no matter what their disability or health condition.
- The Global Gastroschisis Foundation (opens in a new tab) is dedicated to research, awareness, and support for patients and families affected by gastroschisis.
- BLISS (opens in a new tab) provides support, advice and information for the parents and families of babies born prematurely, requiring intensive care and/or special care. They also work with bereaved families.
Chaperoning
During your child’s hospital visits your baby will need to be examined to help diagnose and to plan care.
Examination, which may take place before, during and after treatment, is performed by trained members of staff and will always be explained to you beforehand. A chaperone is a separate member of staff who is present during the examination.
The role of the chaperone is to provide practical assistance with the examination and to provide support to the child, family member/ carer and to the person examining.
Contacts/Further Information
Paediatric surgery clinical nurse specialist team
Office: 01223 586973
(Mon to Fri 08:00 to 18:00 except bank holidays)
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/