Introduction
There are four types of tube used as direct jejunostomy feeding tubes used in Children’s Services at Addenbrooke’s Hospital:
- Vygon (Avanos) direct jejunal tube (most common)
- Fresenius Freka Direct jejunal tube
- Vygon Mic G tube used as a direct jejunal tube
- Balloon (Foley) catheter used as a balloon retained direct jejunal tube

Fresenius Freka Direct Jejunal Tube: Transparent (clear) tubing, inserted during surgery to form a tract, changed after six weeks to balloon retained tube.

Vygon Direct Jejunal Tube: white coloured tubing, inserted during surgery to form a tract, can be left in place as long as required by the child. If displacement occurs; can be replaced at hospital

Vygon Mic G tube: used as a Direct Jejunal Tube: May be used when Fresenius direct tube is electively changed if child's size permits

Balloon (Foley) catheter used as a Direct Jejunal tube: May be used as emergency placement when other brands of direct jejunal tube displaces.
The choice of tube depends upon a number of factors including your child’s size, length of time jejunal feeding is likely to be required for; their level of risk related to anaesthetic, what is technically possible during surgery in your child and the extent to which your child has a tendency to pull on their tube. Your nurse specialists will meet you and show you the types of tube and will teach you how to care for them. This leaflet, which discusses all types of direct jejunal feeding tubes, contains information about tube insertion and tube care as a reference for you. The leaflet has been divided into five sections:
Part 1: General information about what a jejunal feeding tube is, why it has been recommended for your child and the advantages and disadvantages related to this type of feeding tube.
Part 2: Commonly asked questions and general care information applicable to all direct jejunal tubes.
Part 3: Specific care related to the Fresenius Freka Direct jejunal tube.
Part 4: Specific care related to the Vygon (Avanos) direct jejunal tube.
Part 5: Specific care related to the Vygon Mic G tube used as a direct jejunal tube.
Part 6: Specific care related to the Foley catheter when used as a direct jejunal tube.
Part 7: Specific Information about your child’s tube and contact numbers for advice.
Part 1: General information
What is jejunal feeding?
Rather than delivering fluid and food into the stomach, jejunal feeding delivers fluid and nutrition directly into the jejunum. Jejunostomy feeding is a safe and effective method of giving liquid nutrition, fluid and medicines to people who need to be fed in a way that bypasses the stomach.
Where is the jejunum?
The small intestine is part of the gastrointestinal tract between the stomach and the large intestine (also known as the colon). The small intestine is where most of the water nutrients from food are absorbed. The small intestine is divided into three parts:
- The duodenum
- The jejunum
- The ileum

What is a jejunostomy tube and how is it inserted?
A jejunostomy is a surgically made stoma (‘hole’). Whilst your child is receiving a general anaesthetic the surgeon will make a small cut in the abdominal skin (called a ‘mini laparotomy’) and will then be able to see the bowel. A small cut is then made in the jejunum and a tube is then passed through this passage into the jejunum. The skin is then sewn around the tube and the wound closed. The tube will be secured at the skin with a fixation plate which is also sewn in place at skin level. Connectors and clamps are then added to the external tubing before the child is woken from the anaesthetic.
Why is a jejunostomy required?
There are a number of reasons why a child might have a jejunal tube and your doctor and nurse specialist will explain these to you. Some of the common reasons are children:
- Who are at risk of aspiration when they are fed into their stomach which is known as ‘aspiration pneumonia’. Aspiration pneumonia happens when a liquid, such as fluids or food from the stomach, goes into the lungs rather than only down the food pipe and into the stomach.
- Who are too small to have a Nissen’s Fundoplication operation to treat their reflux.
- Who are too unwell to have a Nissen’s Fundoplication to treat their reflux.
- With dysmotility problems and so cannot tolerate gastric feeding (feeding into the stomach).
- Who have had a recurrence of their gastro-oesophageal reflux after a Nissen’s Fundoplication operation and for whom a ‘redo’ Nissen’s Fundoplication is not likely to be in the child’s best interests/helpful.
Part 2: Commonly asked questions and general care information applicable to all direct jejunal tubes:
What are the advantages of a direct jejunostomy tube?
- Ensures the child receives their hydration and nutritional requirements when they are unable to do so by other means.
- Prevents the need for a ‘Naso-jejunal tube’ (a tube which passes via the nose, down the food pipe, into the stomach and then down into the jejunum) which can be less cosmetically pleasing and which are more likely to be accidentally pulled out and, which can be difficult to insert.
- Reduces the risk of aspiration.
- Once your child’s doctors and dieticians have agreed that your child no longer requires their jejunal tube, direct jejunal tubes can be removed without the need for another general anaesthetic.
What are the disadvantages of a direct jejunostomy tube?
- An operation is required to insert the child’s first direct jejunal tube.
- Jejunal feeding has to take place over many hours of the day and night because, unlike the stomach, the jejunum is not a storage organ and so cannot tolerate food boluses. Instead, feed must be slowly dripped into the jejunum. This means that children need to be connected to feeding pumps for long periods of time to slowly administer food and water.
- The tube can be accidentally pulled out with relative ease and so careful attention is needed to ensure that dressings are secure.
- If a tube is accidentally pulled out, the stoma (hole) can close very quickly (within an hour) and so immediate attention must be given regarding insertion of a new tube. Children with jejunal tubes must always carry with them an ‘emergency kit’, which includes all the equipment needed to insert a temporary emergency .
- The tube can get blocked (with feed or medication) and will therefore need replacing. Appropriate flushing of the tube helps to prevent tube blockage.
- The tube is a foreign object in the body and can therefore be associated with infections around the site. Daily cleaning of the surrounding skin helps to prevent this.
- Very rarely the bowel close to the jejunum can twist around the jejunum with the tubing in it causing a serious obstruction within the bowel. Symptoms include pain, vomiting bile (coloured green), distension of the abdomen and a child who appears unwell in themselves. Emergency review is required and surgery is likely to be necessary.
Administering feed/fluids via a jejunostomy tube
Your care team (nutrition specialist/surgical nurse specialist/dietician) will recommend a feeding plan suitable for your child’s needs and will provide teaching for you on how to administer it.
It is important to wash hands thoroughly prior to and after accessing any jejunostomy tube.
It is not necessary to check the position of the tube prior to feeding via it, unless you are concerned that the tube does not have its normal appearance/may have dislodged.
To maintain tube patency (prevent blockage) it is essential that a flush of at least 20mls of sterile water (that is, cooled boiled water) is administered after a feed has been given. (Smaller volumes may be used in exceptional circumstances).
Your care team will teach you how to administer feeds whilst you are in hospital.
Administering medication via a jejunostomy tube
Ideally your child’s medication should be still given into the stomach but, where this is not possible, administration of the medication via the jejunal tube may be necessary.
In circumstances where the jejunal tube is to be used for delivery of medication, discussion must firstly take place with your child’s specialist care team and children’s pharmacist because some medicines need to mix with the acid in the stomach (that is not present in the jejunum) to work, others can block jejunal tubes and others need to be given in different doses when administered into the jejunum compared to the stomach.
Administering medication correctly will ensure that the medicine is absorbed properly. While you are in hospital a children’s pharmacist will review your child’s medicines so you know how best to administer them.
Where medicines are being given through the jejunal tube, the speed of administration should not exceed two to three mls per minute. This is to improve the likelihood of the medicine being absorbed.
Administering medication correctly will also avoid the tube becoming blocked. Usually your child’s medication should be provided in a liquid form but some liquid medications are known to be associated with tube blockages and so need to be further diluted with water (usually the same volume of water as medicine) or another liquid before being given. Ask a member of your specialist care team if you are unsure.
If medication is only available in tablet form, seek advice from your GP, pharmacist or nurse specialist. Some tablets can be crushed or mixed with water but others cannot as their particles can lead to tube blockages.
The tube must be flushed before and after each medicine. If more than one medicine is being given, flush in between as well. The water used should have been boiled and then allowed to cool. It is important to always wash your hands thoroughly before and after using the tube for administration of medication.
Please note, Clarithromycin will block your child’s tube and so should never be given through the tube. This is an antibiotic commonly used for chest infections. Other antibiotics which sound similar (for example Erythromycin) do not usually block tubes.
Procedure for medication administration via a jejunal tube
- Wash hands thoroughly.
- Draw up medications into separate enteral (purple) syringes
- Draw up a flush of water into a separate syringe (this should be sterile water that is, water that has been boiled and allowed to cool)
- Unscrew the cap from the end of the jejunostomy
- Connect syringe with flush in
- Where applicable, release clamp
- Administer approximately 2mls of flush to confirm that the tube is patent (working)
- Where applicable, apply clamp
- Disconnect flush syringe and connect syringe containing medication
- Where applicable, release clamp
- Administer medication at a speed of 2-3mls per minute
- Where applicable, apply clamp
- Disconnect medication and connect syringe containing the flush
- Where applicable, release clamp
- Administer flush
- Repeat steps nine to fifteen for each medication
- Reapply the clamp and screw the cap back on
General Care: Cleaning/skin care
It is expected that there will be a clear/coloured discharge at the stoma site for the first few days (seven to fourteen) until the stoma heals.
Daily care of the stoma site will reduce the possibility of infections.
Always ensure you wash your hands before and after providing any care for a jejunostomy tube/site.
The jejunostomy site should be cleaned daily with warm soapy water. Baths are permitted once the site is fully healed (usually five days after tube insertion). Dry the area thoroughly afterwards.
Always avoid using creams/powders on the skin around the tube unless they have been prescribed by a member of your child’s specialist team as they can damage the tube material and lead to skin irritation/give rise to infection.
Dressings around the jejunostomy tube are required to help hold the tube in place. The jejunal tube should be ‘looped’ under the dressing to help prevent tube displacement if accidently pulled. The dressing applied should be clear so you can see that the loop of tubing is still in place. Dressings will need to be changed daily at the same time as the site is cleaned.
During cleaning of the site and changes of dressing, observe the site for signs of infection such as redness, swelling and pus discharge – see section on infection for further information.
The stitches that are in place should not be removed but instead allowed to displace on their own.
Infection
Daily cleaning of the jejunostomy site will help to reduce the risk of infection (see section on cleaning and skin care).
If you notice that the jejunostomy site is inflamed, red, sore or discharging, contact a member of your care team for advice. Some discharge is to be expected for the first seven to fourteen days after tube insertion and may not represent infection but if you are concerned your child should be seen by one of your care team.
When infection is suspected a swab of the area will be taken to help identify what treatment is needed. Sometimes antibiotic creams can be used but sometimes antibiotics will need to be given via a child’s tube.
Anti-microbial dressings can also be helpful to prevent infection; ask your nurse specialist or community nurse for more information.
Flushing
Flushing the tube is essential to prevent blockages. The jejunostomy tube should be flushed with sterile water (that is, water that has been boiled and then allowed to cool).
Unless otherwise specified by your dietician, a minimum of 20mls of water should be used for flushes after feeds or after medication has been given. Your dietician may advise that, in addition, you give a flush prior to feeding to ensure your child’s fluid requirements are met.
When giving drugs, it is important to flush between each medicine as well as after them to prevent precipitation (settling of the drugs) in the tubing (see section on ‘Administration of Medication’).
Replacing feeding sets
Continuous (‘Pump’) feeding sets should be discarded 24 hours after first use.
Where will I get supplies of the consumable items from?
The children’s nutrition nurse specialist will visit you and ascertain what equipment you need and how much. Before you go home your care team will provide you with an initial seven to fourteen day supply of equipment. In most areas an ongoing supply of equipment can be delivered to your home. Your care team will arrange this while you are still in hospital. If this service is not available in your area, your care team will ensure that alternative arrangements are in place for you. You should remember to order new supplies in good time before you run out and only use equipment for the length of time specified by the manufacturer
What is an ‘emergency kit box?’
Before you leave hospital one of the nurse specialists will provide you with an emergency kit box. This box will contain all the items needed for your child’s tube in the event of the jejunal tube falling out. A copy of this information leaflet will also be provided in the box which has been completed with specific information about your child’s tube.

Can I/my child bath and shower?
Yes, showers and baths are permitted after five days. Always ensure that the tube end is closed and, where applicable, the clamp applied. Dry the area thoroughly afterwards.
Can I/my child go swimming?
Yes! Ensure the tube end is closed and, where applicable, the clamp applied. Make sure to coil the tubing under a waterproof dressing.
Will I or my child be able to go to school?
Your child should be able to go to school as normal. Staff at the school must be taught what to do if the tube falls out and spare supplies should be kept at the school for emergency use.
Can we go on holiday?
It is fine to travel with your child.
It may be helpful, particularly if your child has complex needs, to take a letter with you from your doctor which can help you if you need to seek medical advice whilst on holiday.
Letters from your care team can be useful to prevent any problems with airport security when you are travelling with ‘medical equipment.’
Remember to take extra supplies with you and to pack at least some of these in your hand luggage in case your main luggage goes astray.
Use a large dressing to avoid getting sand near the stoma site as this can irritate the skin.
Your home delivery company may offer to give practical advice.
Problem solving - tube blockage
To prevent tube blockage the tube should be flushed with at least 20mls of water after giving feeds or medication. Always ensure medications are being administered in a way that limits the chances of tube blockage (see section on ‘administering medication’).
If the tube does block you may try the following. If unsuccessful on the first step, try the next:
- Ensure all clamps are open and the tube is not kinked.
- Try to flush using a pumping action with the plunger on the syringe.
- Connect a 20 or 50ml syringe to the end of the tube and try to draw back (aspirate).
- Mix a solution of sodium bicarbonate (baking soda). Mix half a teaspoon of sodium bicarbonate (baking soda) with 30mls of boiling water. Leave this to cool to a warm temperature then use a 10ml syringe to flush this solution down the tube. Leave the solution in the tubing for at least two hours (can be left overnight) then flush it through with 20mls of water.
- If the above does not help, it is advisable to change the tube. (Contact your community nurse or surgical nurse specialist to help with this).
- Discard of equipment safely.
Do not use any of the following items to try and unblock your child’s tube:
- Needles – these can put holes into the tubing or could damage your child’s bowel.
- Wire – this can also put holes into the tubing or could damage your child’s bowel.
- Cola – this can damage the tubing itself
Discharge observed from stoma site
It is usual to experience a small amount of clear discharge at the stoma site until the stoma heals (usually seven to fourteen days after placement). It is important to clean the area carefully during this time. If the discharge is spoiling clothing a small ‘key hole’ dressing can be applied but should be changed regularly/removed when no longer needed.
If the discharge looks like pus your child should be reviewed by a member of their care team as this can be a sign of infection (see section on ‘Infection’ above).
If the discharge appears to be milk, contact a member of your care team.
Sore skin
Redness or soreness around the skin and stoma can occur for many reasons, for example, due to leakage of feed from the jejunal stoma, due to infection or due to friction of the tubing within the tract itself. Clean and dry the area frequently.
Call your community nurse if the stoma is persistently red and sore, the stoma emits an odour, the surrounding skin is swollen, pus is observed or there is bleeding from the site.
Overgranulation
Granulation tissue is the result of the body trying to repair itself. You may recognise overgranulation as a clear brownish discharge and occasional bleeding or as pinkish raised tissue.
If bleeding occurs or a large amount of tissue builds up, contact a member of your gastrostomy care team for advice as treatment may be needed. Where treatment is required this is most commonly in the form of an ointment.
When diarrhoea occurs:
The rate of feeding may need to be slowed down. Liaise with your dietician for advice. If diarrhoea continues contact your doctor.
When vomiting occurs:
You may need to slow the rate of feeding. Liaise with your dietician for advice. Always check expiry dates of feed.
Part 3: Specific care related to the Fresenius Freka direct jejunal tube
Parts of the tubing and their function
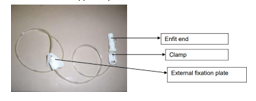
External fixation plate: Keeps the tube’s position next to the skin. There will be two small stitches in the skin and fixation plate helping to hold the tube in place.
Clamp: Prevents feed from coming back up the tube.
Enfit End: Connector which fits into syringes/feeding administration sets by which feed/fluids/medications can be administered.
Stitch removal
At the time of the operation to insert a Fresenius Freka Direct jejunal tube, two stitches are inserted to help hold the tube in place. These stitches should not be removed but will fall out on their own. It is important that dressings are secure, particularly after the stitches have fallen out, to prevent the tube displacing.
Tube change and follow up
A Fresenius Freka Direct jejunal tube is left in place for six weeks whilst the tract heals. Before you leave hospital your nurse specialist will arrange an appointment with you to change the Fresenius Direct jejunal tube. Tube changes are undertaken in our children's outpatient clinic by a member of the nurse specialist team. Changing the tube takes only approximately 10 to 15 minutes but, expect your appointment to last for approximately one hour in total as your nurse specialist will provide further training for you after the tube change and also update your child’s care plan for your emergency kit box.
Problem solving specific to a Fresenius Direct jejunal tube (see section on problem solving above for generic problems)
What to do if your child’s Fresenius direct jejunal tube falls out
- Collect your child’s emergency kit box which will contain all the equipment that you need:
- One clear Luer slip syringe
- One purple enteral syringe
- Silastic Foley catheter of same size as child’s current tube (for example 8Fr)
- Silastic Foley catheter which is one size smaller than your child’s current tube (for example 6Fr)
- Sterile water to inflate balloon
- Water based lubricant (e.g. Water based lubricant)
- One feeding connector (from feeding set)
- Mefix tape/equivalent
- Tegaderm dressing
- pH paper
- Draw up _____mls of sterile water into the syringe provided
- Lubricate the 8Fr Silastic Foley catheter with the water based lubricant
- Gently push 2cms of the catheter into the jejunal tract
- Where applicable, remove the introducer from the catheter
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further 2cms. If no bile is seen, ensure you insert at least half of the length of the tubing
- Inflate the balloon with _____ mls of sterile water previously drawn up
- Check pH to confirm position using the purple enteral syringe. If aspiration is difficult, place the tube on free drainage for 30 minutes and check pH of free drainage fluid. (pH should be six to eight)
- pH must be confirmed before feeding is recommenced
- Wipe any residual lubricant from skin
- Secure in place by making a loop in the tubing then taping the loop in place with two strips of Mefix
- Cover with a transparent (Tegaderm) dressing
- Apply feeding connector and bung
- Discard of equipment safely
- As your child’s jejunal tube has been in place for less than six weeks, your child must be seen in an Emergency Department and an x-ray taken to confirm tube position before feeding is recommenced
- Update the Clinical Nurse Specialist team so that further training can be arranged regarding elective tube changes.
Notes
- If resistance is felt on passing the tube, remove and re try. Do not exert force as this may perforate the bowel.
- If the 8Fr catheter cannot be inserted, use a 6 Fr instead and inform the paediatric surgery team.
- pH must be confirmed and an x-ray taken to confirm position of the new tube when your child is within the first six weeks of having had their operation to insert their Fresenius Freka Direct jejunal tube.
Leakage of feed is observed from the stoma site
Leakage of milk feed may be observed coming from the stoma site if the tube is not far enough down the jejunum. Assess whether the fixation plate is still at skin level and the length of the tubing. Call the nurse specialist team for advice.
The tubing appears shorter than normal
If your child’s jejunal tube is not held securely with a dressing at skin level, the jejunal tube can migrate inside in the bowel. Keeping dressings in place and secure is therefore very important.
You will quickly learn what the normal appearance of your child’s jejunal tube is. If you notice that the tube appears shorter than usual you will need to gently pull the tube back to its normal position and then secure with a new dressing. If you are unsure, contact a member of your child’s care team.
Part 4: Specific care related to the Vygon (Avanos) direct jejunal tube
Parts of the tubing and their function
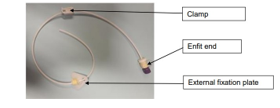
External fixation plate: Keeps the tube’s position next to the skin. There will be a dressing covering this to help hold the tube in place.
Clamp: Prevents feed from coming back up the tube.
Enfit End: Connector which fits into syringes/feeding administration sets by which feed/fluids/medications can be administered.
Tube change and follow up
A Vygon (Avanos) Direct jejunal tube can be left in place for as long as it is clinically required and for as long as the tube’s condition remains free of problems. If problems occur such as increased difficulty flushing the device, holes in the tubing or insecure fit of connectors, you should contact your nurse specialist team for review and planned tube change at the hospital.
Problem solving specific to a Vygon (Avanos) Direct jejunal tube (see section on problem solving above for generic problems)
What to do if your child’s Vygon (Avanos) direct jejunal tube falls out
- Collect your child’s emergency kit box which will contain all the equipment that you need:
- One clear Luer slip syringe
- One purple enteral syringe
- Silastic Foley catheter of same size as child’s current tube (for example 8Fr)
- Silastic Foley catheter which is one size smaller than your child’s current tube (for example 6Fr)
- Sterile water to inflate balloon
- Water based lubricant
- One feeding connector (from feeding set)
- Mefix tape/equivalent
- Tegaderm dressing
- pH paper
- Draw up _____mls of sterile water into the syringe provided
- Lubricate the 8Fr Silastic Foley catheter with the water based lubricant
- Gently push _____cm of the catheter into the jejunal tract
- Where applicable, remove the introducer from the catheter
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further 2cms. If no bile is seen, ensure you insert at least half of the length of the tubing
- Inflate the balloon with _____ mls of sterile water previously drawn up
- Check pH to confirm position using the purple enteral syringe. If aspiration is difficult, place the tube on free drainage for 30 minutes and check pH of free drainage fluid. (pH should be six to eight)
- pH must be confirmed before feeding is recommenced
- Wipe any residual water based lubricant from skin
- Secure in place by making a loop in the tubing then taping the loop in place with two strips of Mefix
- Cover with a transparent (Tegaderm) dressing
- Apply feeding connector and bung
- Discard of equipment safely
- If your child’s jejunal tube has been in place for less than six weeks, your child should be seen in an Emergency Department and an x-ray taken to confirm tube position before feeding is recommenced
- If your child’s jejunal tube has been in place for more than 6 weeks and appropriate position has been confirmed on pH testing this tube can be used for feeding temporarily
- Update the Clinical Nurse Specialist team so a date and time for reinsertion of a new Vygon (Avanos) direct jejunal tube can be arranged.
- Parents/carers need to retain the displaced tube with the fixation plate and bring to the appointment with the Clinical Nurse Specialist
Notes
- If resistance is felt on passing the tube, remove and re try. Do not exert force as this may perforate the bowel.
- If the 8Fr catheter cannot be inserted, use a 6 Fr instead and inform the paediatric surgery team.
- pH must be confirmed and an x-ray taken to confirm position of the new tube when your child is within the first six weeks of having had their original operation.
Leakage of feed is observed from the stoma site
Leakage of milk feed may be observed coming from the stoma site if the tube is not far enough down the jejunum. Assess whether the fixation plate is still at skin level and the length of the tubing. Call the nurse specialist team for advice.
The tubing appears shorter than normal
If your child’s jejunal tube is not held securely with a dressing at skin level, the jejunal tube can migrate inside in the bowel. Keeping dressings in place and secure is therefore very important.
You will quickly learn what the normal appearance of your child’s jejunal tube is. If you notice that the tube appears shorter than usual you will need to gently pull the tube back to its normal position and then secure with a new dressing. If you are unsure, contact a member of your child’s care team.
Part 5: Specific care related to the Vygon (Avanos) Mic G tube when used as a direct jejunal tube
Parts of the tubing and their function:
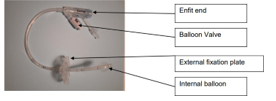
Internal balloon: To prevent tube displacement.
Enfit End: To enable the use of enteral feeding equipment.
External fixation plate: To help secure tube at skin level
Balloon valve: To permit access to the retaining balloon.
Vygon (Avanos) Mic G tubes are manufactured for use as gastrostomy tubes and thus, for use in children’s stomach’s rather than their bowels. The ‘off-label’ use of a Mic G tube as a direct jejunal tube may be advised for your child to, for example, prevent repeat general anaesthetics and promote community based care.
Elective changes of a balloon retained direct jejunal tube
Mic G tubes, when used as balloon retained direct jejunal tubes should be changed every 8 to 12 weeks. It is important that tube changes take place in as clean an environment as possible to prevent infection.
Until you are both competent and confident to change the tube yourself, your child’s community children’s nurse will be present to support the tube changes and provide teaching for you. If your child’s community nurse is not experienced in changing jejunal tubes then training for you and your child’s community nurse will be provided by the surgical clinical nurse specialists at Addenbrookes Hospital.
Procedure for an elective (planned) balloon retained jejunal tube change:
- Collect equipment:
- Clean tray (to lay equipment on when opened)
- Dressing Pack
- Sterile gloves
- one sachet of Sodium Chloride for cleaning skin
- two clear Luer slip syringes (2.5 or 5ml)
- one purple enteral syringe
- Mic G tube of same size as child’s current tube (for example 12Fr)
- Mic G or Silastic Foley catheter which is one size smaller than your child’s current tube (for example 10Fr)
- Sterile water ampoule
- Lubricating Jelly
- Mefix Tape/equivalent
- Tegaderm dressing/equivalent
- Zoff/equivalent to remove old dressing
- Wash hands thoroughly
- Open corner of dressing pack and peel outer covering apart, drop the dressing pack itself onto the tray
- With minimal handling, open the corners of the dressing pack out to reveal the contents
- Pour the Sodium chloride from the sachet into one of the compartments of the tray in the dressing pack
- Pour approx. 5mls of sterile (cool, boiled) water into another of the compartments of the tray
- Open and drop the two syringes onto the sterile area
- Open and drop the new Mic G tube onto the sterile area
- Without touching the sterile area, pour a small amount of lubricating jelly onto the edge of the sterile area
- Prepare two strips of Mefix tape and Tegaderm dressing
- Remove old dressing
- Wash hands again
- Put on gloves
- Move the external fixation plate away from the internal balloon
- Draw up _____ ml of sterile water into one of the syringes
- Soak three pieces of gauze with the sodium chloride
- Wipe around the jejunal stoma site once in a clockwise direction and then discard the piece of gauze. Repeat three times
- Use fourth gauze square to dry site
- Lay the dressing towel next to your child to create a clean area for laying the new jejunal tube if desired
- Using the empty syringe deflate the balloon on the jejunal tube and note how much water is removed (for example 0.5 ml is often lost between each change)
- Gently pull on the jejunal tube until it has been completely removed
- Lubricate the new jejunal tube (Mic G) with the lubricating jelly and then gently push ______cm of tubing into the jejunal stoma.
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further two cm. (This means that at least half of the tubing has usually been inserted into the tract but it may be necessary to insert the entire length of tubing)
- If a tube of the same size as your child’s previous tube cannot be inserted, insert a tube which is one size smaller and update your Paediatric Surgery Nurse Specialist.
- Inflate the balloon with ___ ml of sterile water previously drawn up into one of the syringes
- Gently slide the external fixation plate down to skin level.
- Check pH to confirm position using the purple enteral syringe. If aspiration is difficult, place the tube on free drainage for 30 minutes and check pH of free drainage fluid. (pH should be six to eight). The tube can be placed on free drainage using a syringe; pull the plunger on the syringe back as far as possible and then connect the syringe onto the jejunal connector.
- pH must be confirmed before feeding is recommenced.
- Wipe any residual lubricating jelly from the skin with the last piece of clean gauze
- Secure in place with two strips of Mefix which is wound around the tube and then onto the skin
- Cover with a transparent for (example Tegaderm) dressing
- Discard of equipment safely
- Document date of tube change so that the date of the next change being due can be worked out (every four weeks)
- Contact your home delivery company and community nurses regarding replacement items.
Changes of water from the internal retaining balloon
The water in the retaining balloon needs to be changed once per week.
The purpose of changing the water is to ascertain the condition of the balloon. If the balloon is beginning to perish, this will be indicated by either aspirating less water than expected and/or the water which is aspirated being discoloured. If either of these signs are observed you should arrange for your child’s tube to be changed within 24 hours. If these signs are ignored the balloon is at risk of rupturing and the tube may then fall out.
Procedure for changing the water in the balloon:
- Collect equipment two clear Luer slip syringes 2.5ml or 5ml, sterile (cooled boiled) water
- Wash hands
- Ensure that the dressing on the tubing is secure. If this is not secure you must perform a dressing change before changing the water in the retaining balloon to prevent accidental displacement of the tube during the water change.
- Draw up_____ mls of water into one of the syringes
- Insert the empty syringe into the balloon valve
- Aspirate the water out
- Check the aspirated water in the syringe for volume and colour. Remember, it is common for 0.5 ml of water to be lost from the balloon each week but if more than this is lost the balloon may be perishing.
- Discard this old water
- Pick up the syringe containing the new water. Push the syringe into the balloon valve and let go of the syringe. If the syringe has been inserted correctly it will stay connected to the tube on release. Inject the water.
- Once all the water has been injected, remove the syringe using a slight twisting motion. It is important to keep your thumb on the end of the syringe whilst removing it to prevent water being expelled back into the syringe spontaneously.
Problem solving specific to a Mic G tube used as a direct Jejunal tube (see section on problem solving above for generic problems)
The jejunostomy tube has fallen out
Emergency replacement of the jejunal tube must be carried out immediately as the hole can start to close within one hour.
- Collect together equipment required from your child’s emergency kit box:
- One 5 ml clear Luer slip syringe
- One purple enteral syringe
- Mic G tube of same size as child’s current tube (e.g. 12Fr)
- Mic G or Silastic Foley catheter which is one size smaller than your child’s current tube (e.g. 10Fr)
- Sterile water to inflate balloon
- Water based lubricant
- Mefix tape
- Tegaderm dressing
- pH paper
- Draw up _____ml of sterile water into the syringe provided
- Lubricate the Mic G tube with the water based lubricant
- Gently push the catheter ______cm into the jejunal tract
- Where applicable, remove the introducer from the catheter
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further 2.0cms. If no bile is seen, ensure you insert at least half of the length of the tubing
- Inflate the balloon with _____ mls of sterile water previously drawn up
- Check pH to confirm position. If aspiration is difficult, place the tube on free drainage for 30 minutes and check pH of free drainage fluid. (pH should be six to eight)
- pH MUST be confirmed before feeding is recommenced
- Wipe any residual water based lubricant from skin
- Secure in place by making a loop in the tubing then taping the loop in place with two strips of Mefix
- Cover with a transparent (Tegaderm) dressing
- Apply feeding connector and bung
- Discard of equipment safely
- Document today’s date so that the date of the next change being due can be worked out
- Contact your home delivery company and community nurses regarding replacement items for your child’s emergency kit bag.
Notes
- If resistance is felt on passing the tube, remove and re-try. Do not exert force as this may perforate the bowel
- If the 12Fr Mic G tube cannot be inserted, use a 10Fr Mic G or Foley (balloon) catheter instead and inform the Paediatric Surgery Team
Leakage of feed is observed from the stoma site
Leakage of milk feed may be observed coming from the stoma site when the balloon has started to deflate/completely deflated so firstly, perform a change of water in the retaining balloon (see separate section for procedure)
Leakage of milk may also occur because your child now requires more water in their retaining balloon than they previously required (for example, because they have grown). Before adding a larger volume of water than that which was originally recommended you must liaise with your paediatric surgery nurse specialist for advice. Adding too much water can cause an obstruction within the bowel and so volumes of water for retaining balloons need to be carefully considered.
The tubing appears shorter than normal
If your child’s jejunal tube is not held securely with a dressing at skin level, the jejunal tube can migrate inside in the bowel. Keeping dressings in place and secure is therefore very important.
You will quickly learn what the normal appearance of your child’s jejunal tube is. If you notice that the tube appears shorter than usual you will need to gently pull the tube back to its normal position and then secure with a new dressing. If you are unsure, contact a member of your child’s care team.
The balloon will not deflate
If you cannot extract water from the retaining balloon with the syringe follow these steps:
- Ensure the syringe has been inserted correctly. If the syringe has been pushed in too far or not far enough, water will not be expelled from the balloon.
- Ensure the recess in the balloon valve is clean. Occasionally this recess can trap spills of feed or other material. Clean inside the recess with warm water (cotton buds are useful for this) then try to insert the syringe again.
- If the balloon will still not deflate you should contact your community nurse or paediatric surgery nurse specialist.
Part 6: Specific care related to a Foley catheter used as a direct jejunal tube
Parts of the tubing and their function:
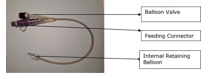
Internal balloon: To prevent tube displacement.
Feeding connector: To enable the use of enteral feeding equipment.
Balloon valve: To permit access to the retaining balloon.
Foley (balloon) catheters are manufactured for use catheters in the bladder. The ‘off-label’ use of a foley catheter as a direct jejunal tube may be advised for your child in an emergency situation (for example if their regular type of jejunal tube has displaced or, in rare circumstances, due to their size and has been subject to a rigorous risk assessment by your child’s care team.
Elective changes of a balloon retained direct jejunal tube
Balloon retained direct jejunal tubes should be changed every four weeks. It is important that tube changes take place in as clean an environment as possible to prevent infection.
Until you are both competent and confident to change the tube yourself, your child’s community children’s nurse will be present to support the tube changes and provide teaching for you.
If your child’s community nurse is not experienced in changing jejunal tubes then training for you and your child’s community nurse will be provided by the surgical clinical nurse specialists at Addenbrookes Hospital.
Procedure for an elective (planned) balloon retained jejunal tube change:
- Collect equipment:
- Clean tray (to lay equipment on when opened)
- Dressing Pack
- Sterile gloves
- one sachet of Sodium Chloride cleaning skin
- two clear Luer slip syringes (2.5 or 5ml)
- one purple enteral syringe
- Silastic Foley catheter of same size as child’s current tube (for example 8Fr)
- Silastic Foley catheter which is one size smaller than your child’s current tube (for example 6Fr)
- Sterile water ampoule
- Lubricating Jelly
- one feeding connector (from feeding set)
- Mefix Tape/equivalent
- Tegaderm dressing/equivalent
- Zoff/equivalent to remove old dressing
- Wash hands thoroughly
- Open corner of dressing pack and peel outer covering apart, drop the dressing pack itself onto the tray
- With minimal handling, open the corners of the dressing pack out to reveal the contents
- Pour the Sodium chloride from the sachet into one of the compartments of the tray in the dressing pack
- Pour approx 5mls of sterile (cool, boiled) water into another of the compartments of the tray
- Open and drop the two syringes onto the sterile area
- Open and drop the catheter onto the sterile area
- Without touching the sterile area, pour a small amount of lubricating jelly onto the edge of the sterile area
- Prepare two strips of Mefix tape and Tegaderm dressing
- Remove old dressing
- Wash hands again
- Put on gloves
- Draw up _____ ml of sterile water into one of the syringes
- Soak three pieces of gauze with the sodium chloride
- Wipe around the jejunal stoma site once in a clockwise direction and then discard the piece of gauze. Repeat three times
- Use fourth gauze square to dry site
- Lay the dressing towel next to your child to create a clean area for laying the new jejunal tube if desired
- Using the empty syringe deflate the balloon on the jejunal tube and note how much water is removed (for example 0.5 ml is often lost between each change)
- Gently pull on the jejunal tube until it has been completely removed
- Lubricate the new jejunal tube (Foley catheter) with the lubricating jelly and then gently push 2cms of tubing into the jejunal stoma.
- Where applicable, remove the introducer from the catheter
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further two cms. (This means that at least half of the tubing has usually been inserted into the tract but it may be necessary to insert the entire length of tubing)
- If a tube of the same size as your child’s previous tube cannot be inserted, insert a tube which is one size smaller and update your Paediatric Surgery Nurse Specialist.
- Inflate the balloon with ___ ml of sterile water previously drawn up into one of the syringes
- Check pH to confirm position using the purple enteral syringe. If aspiration is difficult, place the tube on free drainage for 30 mins and check pH of free drainage fluid. (pH should be six to eight)
- pH must be confirmed before feeding is recommenced.
- Wipe any residual lubricating jelly from the skin with the last piece of clean gauze
- Secure in place with two strips of Mefix which is wound around the tube and then onto the skin
- Cover with a transparent for (example Tegaderm) dressing
- Discard of equipment safely
- Document date of tube change so that the date of the next change being due can be worked out (every four weeks)
- Contact your home delivery company and community nurses regarding replacement items.
Changes of water from the internal retaining balloon
The water in the retaining balloon needs to be changed once per week.
The purpose of changing the water is to ascertain the condition of the balloon. If the balloon is beginning to perish, this will be indicated by either aspirating less water than expected and/or the water which is aspirated being discoloured. If either of these signs are observed you should arrange for your child’s tube to be changed within 24 hours. If these signs are ignored the balloon is at risk of rupturing and the tube may then fall out.
Procedure for changing the water in the balloon:
- Collect equipment two clear Luer slip syringes 2.5ml or 5ml, sterile (cooled boiled) water
- Wash hands
- Ensure that the dressing on the tubing is secure. If this is not secure you must perform a dressing change before changing the water in the retaining balloon to prevent accidental displacement of the tube during the water change.
- Draw up_____ mls of water into one of the syringes
- Insert the empty syringe into the balloon valve
- Aspirate the water out
- Check the aspirated water in the syringe for volume and colour. Remember, it is common for 0.5 ml of water to be lost from the balloon each week but if more than this is lost the balloon may be perishing.
- Discard this old water
- Pick up the syringe containing the new water. Push the syringe into the balloon valve and let go of the syringe. If the syringe has been inserted correctly it will stay connected to the tube on release. Inject the water.
- Once all the water has been injected, remove the syringe using a slight twisting motion. It is important to keep your thumb on the end of the syringe whilst removing it to prevent water being expelled back into the syringe spontaneously.
Problem solving specific to a Foley catheter used as a balloon Retained Direct Jejunal tube (see section on problem solving above for generic problems)
The jejunostomy tube has fallen out
Emergency replacement of the jejunal tube must be carried out immediately as the hole can start to close within one hour.
- Collect together equipment required from your child’s emergency kit bag:
- One 5 ml clear Luer slip syringe
- One purple enteral syringe
- Silastic Foley catheter of same size as child’s current tube (e.g. 8Fr)
- Silastic Foley catheter which is one size smaller than your child’s current tube (e.g. 6Fr)
- Sterile water to inflate balloon
- Water based lubricant
- One feeding connector (from feeding set)
- Mefix tape/equivalent
- Tegaderm dressing
- pH paper
- Draw up _____ml of sterile water into the syringe provided
- Lubricate the 8Fr Silastic Foley catheter with the water based lubricant
- Gently push the catheter 2cms into the jejunal tract
- Where applicable, remove the introducer from the catheter
- Continue to insert the catheter until bile is observed coming into the tube, then insert a further 2.0cms. If no bile is seen, ensure you insert at least half of the length of the tubing
- Inflate the balloon with _____ mls of sterile water previously drawn up
- Check pH to confirm position. If aspiration is difficult, place the tube on free drainage for 30 minutes and check pH of free drainage fluid. (pH should be six to eight)
- pH MUST be confirmed before feeding is recommenced
- Wipe any residual water based lubricant from skin
- Secure in place by making a loop in the tubing then taping the loop in place with two strips of Mefix
- Cover with a transparent (Tegaderm) dressing
- Apply feeding connector and bung
- Discard of equipment safely
- Document today’s date so that the date of the next change being due can be worked out (balloon retained jejunal tubes are changed every four weeks)
- Contact your home delivery company and community nurses regarding replacement items for your child’s emergency kit bag.
Notes
- If resistance is felt on passing the tube, remove and re-try. Do not exert force as this may perforate the bowel
- If the 8Fr catheter cannot be inserted, use a 6Fr instead and inform the Paediatric Surgery Team
Leakage of feed is observed from the stoma site
Leakage of milk feed may be observed coming from the stoma site when the balloon has started to deflate/completely deflated so firstly, perform a change of water in the retaining balloon (see separate section for procedure).
Leakage of milk may also occur because your child now requires more water in their retaining balloon than they previously required (for example, because they have grown). Before adding a larger volume of water than that which was originally recommended you must liaise with your paediatric surgery nurse specialist for advice. Adding too much water can cause an obstruction within the bowel and so volumes of water for retaining balloons need to be carefully considered.
The tubing appears shorter than normal
If your child’s jejunal tube is not held securely with a dressing at skin level, the jejunal tube can migrate inside in the bowel. Keeping dressings in place and secure is therefore very important.
You will quickly learn what the normal appearance of your child’s jejunal tube is. If you notice that the tube appears shorter than usual you will need to gently pull the tube back to its normal position and then secure with a new dressing. If you are unsure, contact a member of your child’s care team.
The balloon will not deflate
If you cannot extract water from the retaining balloon with the syringe follow these steps:
- Ensure the syringe has been inserted correctly. If the syringe has been pushed in too far or not far enough, water will not be expelled from the balloon.
- Ensure the recess in the balloon valve is clean. Occasionally this recess can trap spills of feed or other material. Clean inside the recess with warm water (cotton buds are useful for this) then try to insert the syringe again.
- If the balloon will still not deflate you should contact your community nurse or paediatric surgery nurse specialist.
The connector at the end of the tubing keeps displacing.
To obtain a good seal between the tubing and the feeding connector, and so prevent the connector from displacing, two dry surfaces are required. Remove the feeding connector and dry the connector thoroughly. By using a piece of tissue, thoroughly dry the inside of the tubing. Replace the connector.
If the problem persists contact your community nurse or paediatric surgery clinical nurse specialist for advice.
Part 7: Details of your/your child’s jejunostomy tube
|
Type of direct jejunal tube |
|
|---|---|
| Insertion date | |
| Brand of tube | |
| Size of tube | |
|
Elective change of tube due |
| Position | Name | Contact number |
|---|---|---|
|
Position
Nurse specialist (paediatric general surgery) Monday to Friday 08:00 to 18:00 |
Name |
Contact number
Office (calls are returned on same working day): 01223 586973 |
|
Position
On-call paediatric surgery registrar (out of working hours) |
Name |
Contact number
For out of hours emergencies: 01223 245151 and ask switchboard staff to “contact the on call paediatric surgery registrar” |
| Position Nutrition nurse specialist | Name | Contact number |
| Position Dietician | Name | Contact number |
|
Position
Community paediatric nurse |
Name | Contact number |
| Position Home delivery company | Name | Contact number |
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/