Introduction
This leaflet has been written to provide information to parents and families whose baby has been diagnosed with a cystic lung lesion and aims to support the discussion you have had with your baby’s consultant and team.
What is a congenital cystic lung lesion?
A congenital cystic lung lesion is an uncommon condition in which abnormal lung tissue forms a cyst or a solid mass within the baby’s lung during pregnancy. This section of abnormal lung tissue does not function normally. The cyst or mass is benign (not cancerous) but does continue to grow. Approximately one in every 10,000 babies born have a congenital lung lesion.
There are three types:
- Congenital Pulmonary Airway Malformation (CPAM) – most common type
- Congenital Lobar Emphysema (CLE) - rare
- Bronchopulmonary Sequestration (BPS) - rare
This leaflet gives information on CPAM. The diagram below shows a CPAM, the most common cystic lesion. Some babies with CPAM will also have a build-up of fluid in their abdomen (tummy) which is called ‘hydrops’ or 'ascites' and is shown in the diagram below.
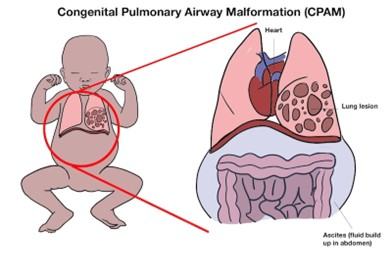
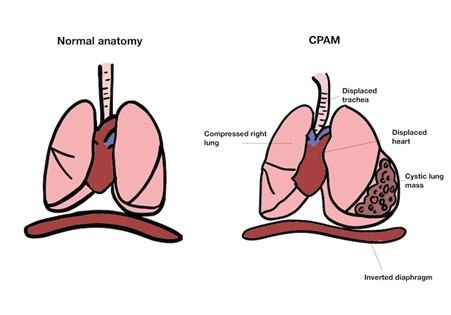
The presence of the CPAM can mean that other organs, such as the heart and trachea (windpipe), get pushed out of their normal position and the unaffected lung can get squeezed (compressed) as shown in the diagram below:
What causes cystic lung lesions?
We do not know what causes these lesions to occur, and there is no link between anything that happened during pregnancy and these conditions. These problems are not known to be linked to any genetic conditions and do not run in families.
Signs and symptoms
CPAMs can be detected during routine scans during pregnancy. Most lesions are small and do not cause any stress to your baby’s heart before birth. Rarely, these areas of tissue grow to be a significant size and the flow of blood around the baby’s body is affected. This leads to an excessive amount of fluid building in the baby’s body which is called ’fetal hydrops’.
Where a cystic lung lesion is seen, you will continue to have ultrasound scans throughout the pregnancy, to monitor for complications such as heart failure and fetal hydrops. If you and your baby remain well, you should be able to have a normal vaginal delivery. If your baby develops hydrops your pregnancy will be carefully monitored for complications such as high blood pressure and other signs of preeclampsia.
What happens after birth?
When a cystic lung lesion has been seen on a baby during pregnancy we advise that the baby is born at the hospital so that there is access to a paediatric surgical team without delay, if needed. A neonatal doctor will be present at the time of birth to assess your baby.
In the majority of cases, babies will not have breathing problems and they will be able to join you on the postnatal ward. In this scenario, after your baby has been born the amount of oxygen in their blood will be monitored with a small, non-invasive machine called an oxygen saturation monitor and a chest X-ray will be taken. After a period of monitoring and establishing feeds, most babies will go home and have routine maternity care. A Computed Tomography (CT) scan which uses X-rays and a computer to create detailed cross-sectional images (slices) of the inside of the body) will be arranged to look at the chest, which will take place as an outpatient when your baby is 3-4 months old. Following the CT imaging, your baby will be seen in the outpatient children’s chest clinic (called the ‘thoracic clinic’) to discuss a surgical plan.
Sometimes babies show signs of breathing difficulties after being born and are not able to get sufficient oxygen into their body. In these cases, the baby needs to be admitted to the neonatal unit for monitoring and occasionally for help with their breathing. Urgent X-rays are performed. Sometimes air gets stuck in the lungs because it's hard to exhale fully (called ‘air trapping’) and if this is seen on the X-ray, CT imaging and surgical assessment will be arranged without delay.
Treatment and Management
Most commonly surgery will be performed in the first two years of life. The reasons for the operation are mainly preventative:
- To avoid infections.
- To remove the non-functioning part of the lung at a time where there is still compensatory lung growth.
- Avoid the rare risk of future cancer formation.
Planned surgery will be offered using a keyhole approach. There is a small risk of this not being possible, in which case open surgery will be performed. Where surgery has been needed very soon after birth because of breathing problems, the operation is usually open and not keyhole.
What happens after the operation?
Many children born with CPAM, especially those diagnosed during pregnancy, grow to live normal lives. Around 5% of cases develop rarer complications which unfortunately cannot be predicted.
More information about the neonatal unit
Parents are allowed to visit at all times, but there is limited accommodation available for parents of babies on the Neonatal Unit. We try to provide accommodation around the time of admission, surgery and in preparation for discharge home. If you would like to visit the Rosie neonatal unit prior to delivery, please ask the fetal medicine team to contact Neonatal Intensive Care Unit (NICU) to arrange this. A short video introducing the NICU is also available in the Neonatal Services section of the Rosie Hospital website.
Support for you and your child with a cystic lung lesion
- Contact a Family (opens in a new tab) is a UK-wide charity providing advice, information and support to the parents of all disabled children - no matter what their disability or health condition.
- The Congenital Diaphragmatic Hernia Support Charity (opens in a new tab) (CDH UK) provides complementary care to patients and their families in the form of information, emotional and practical support.
- Asthma + Lung UK is a national charity dedicated to better understanding, research, treatment and support for patients with lung conditions. They have a dedicated page for CPAM (opens in a new tab) support.
- BLISS (opens in a new tab) provides support, advice and information for the parents and families of babies born prematurely, requiring intensive care and/or special care. They also work with bereaved families.
Chaperoning
During your child’s hospital visits your baby will need to be examined to help diagnose and to plan care.
Examination, which may take place before, during and after treatment, is performed by trained members of staff and will always be explained to you beforehand. A chaperone is a separate member of staff who is present during the examination.
The role of the chaperone is to provide practical assistance with the examination and to provide support to the child, family member/carer and to the person examining.
Contacts/Further Information
Paediatric surgery clinical nurse specialist team
Office: 01223 586973
(Mon to Fri 08:00 to 18:00 except bank holidays)
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/