What is CADASIL?
CADASIL is an abbreviation for a long name describing a rare heritable form of stroke (Cerebral Autosomal Dominant Arteriopathy with Subcortical Infarcts and Leukoencephalopathy). The disease usually presents with multiple small strokes, and/or migraine. CADASIL is caused by an abnormality (mutation) in a gene called NOTCH3.
What does genetic mean?
In many diseases genetic factors are important. This means that part, or all of the risk, is passed down from one’s parents. Certain diseases are caused by an abnormality in one single gene and CADASIL is one of these diseases. Genes produce proteins, which are necessary for normal functioning of the body. Everybody has two copies of each gene, one passed down from their mother, and one from their father.

In CADASIL, an abnormality in one of these two copies results in the disease. We refer to this as autosomal dominant inheritance. A consequence of this is that if you have CADASIL, you have one normal copy and one abnormal copy of the gene. If you have a child, he or she will receive one copy of the gene from you, and one from your partner. Therefore, there is a 50/50 chance that any child of yours will inherit the abnormal copy of the CADASIL gene and will be at risk of developing CADASIL.
What causes CADASIL?
CADASIL results from an abnormality in a gene known as NOTCH3. This results in production of an abnormal NOTCH3 protein which forms aggregates in the wall of the blood vessels. This results in the small brain blood vessels not functioning quite normally,
leading to reduced brain blood flow, and an inability of the small blood vessels to regulate blood flow.
Although abnormalities in blood vessels can be found throughout the body, they are most severe in the brain, and only produce problems noticed by the person with CADASIL within the brain.

What are the features of the disease?
Most people with the disease will suffer from strokes. These most commonly first occur in the 40s to 70s. Recent data has shown that the average age of first stroke in the UK is increasing and is now 60 years of age. However, the disease can be very variable even within the same family. In some people, no problems may occur until their 60s or 70s, and we are seeing an increasing number of individuals identified with CADASIL who remain well into their 70s.The strokes are what we refer to as lacunar strokes (literally meaning a small lake or hole in the brain). Because they are small, they tend to be fairly mild and individuals often recover well. The most common type of stroke causes weakness affecting one side of the body, which is most often arm or leg weakness, or slurring of speech. If recurrent strokes occur, this can lead to persistent disability.
Migraine is another common feature of CADASIL. This most commonly starts in the 20s but the age of onset is variable. Usually it is what we call ‘complex’ migraine. This means that, in addition to the headache, there are aura, which are short-lived neurological symptoms, most commonly disturbance of vision, numbness down one side of the body, or speech disturbance. We know that migraine, while it can be distressing and painful, is not associated with any worsening of the disease or brain damage.
Individuals with CADASIL can suffer from anxiety or depression. Not surprisingly, depression is very frequent after any type of stroke and usually improves with time, although treatment may be necessary.
Over time, as the disease progresses, cognitive (memory and other ‘thinking’) problems may occur. As people get older dementia may occur. Recent data showed that the average age of onset of dementia in CADASIL in the UK is 74 years.
One unusual feature is of the onset of confusion and reduced consciousness over a period of hours or days, sometimes with fever and seizures; this often follows a migraine attack. This is known as encephalopathy. It recovers completely over 1 to 3 weeks and usually has no long-term effect on the course of the disease.

Investigations when CADASIL is suspected
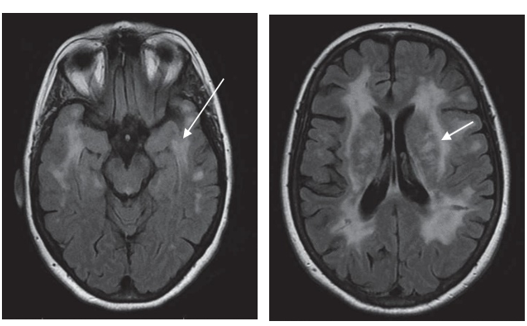
Brain Scans
A magnetic resonance imaging brain scan (MRI) is usually performed and shows characteristic appearances with abnormalities in the deeper parts of the brain known as the white matter. Involvement of certain brain areas, including a region called the anterior temporal lobe, is a useful guide to the diagnosis. This is a safe scan that involves no radiation but some people find it claustrophobic.

Genetic Testing
A definite diagnosis of CADASIL is made on genetic testing. This is done using a small blood sample. If we detect an abnormality on genetic testing, we can be 100% sure that someone has CADASIL. In CADASIL the abnormalities that occur are all within one gene which is called NOTCH3.There are other genes which produce a similar disease to CADASIL- the next most common gene is HTRA1 which causes a disease called CADASIL2. Increasingly, we use a type of genetic testing called next generation sequencing, which tests all the genes which can cause CADASIL-like disease at the same time.
If one member of a family has CADASIL, any other member of the same family who also has CADASIL will have exactly the same underlying genetic abnormality. Therefore, once we’ve found the underlying abnormality within a particular individual, it is relatively easy to determine whether other family members are affected or may become affected in the future.
Skin Biopsy
CADASIL results in characteristic changes in the blood vessels. For obvious reasons it is difficult to look at the blood vessels within the brain. However, even though CADASIL itself only produces symptoms within the brain, abnormalities within the blood vessels can be seen elsewhere in the body. The easiest place to look for these is in the skin. A very small skin biopsy can be performed using local anaesthetic. This can be carried out as an outpatient procedure. We then look at it under high magnification using an electron microscope; in CADASIL one can frequently see abnormal collections of material called GOM (Granular Osmiophilic Material). Because genetic testing will give a definite diagnosis, we only perform skin biopsy if the genetic testing has been negative and the diagnosis is still uncertain.
Cognitive Testing and Neuropsychology
To assess the presence and extent of any cognitive problems we may perform a brief cognitive test in clinic. This usually takes about 10 minutes. In some cases, you may be referred to a clinical neuropsychologist. They will ask you to carry out some more detailed tests to assess your cognitive and thinking abilities. They can then produce skilled advice on how best to manage any cognitive and/or psychological symptoms.
Is there any treatment for CADASIL?
There is no specific treatment for CADASIL available at the moment. In the long run, we hope that a better understanding of how the underlying genetic abnormality causes CADASIL will allow us to discover how this results in the blood vessel damage, and lead to the development of drugs to prevent this damage. However, this is likely to be a number of years away.
The most important thing is to control other risk factors for common stroke. Many studies have shown these risk factors accelerate the damage caused by the CADASIL gene. For example, people with the CADASIL gene who smoke have stroke about 10 years earlier, while those with high blood pressure have about double the risk of stroke. It is important to address these in midlife, before symptoms of CADASIL occur. We recommend an active lifestyle with regular exercise and avoiding being overweight, as well as monitoring of blood pressure and monitoring for diabetes.
Aspirin has been shown to reduce the risk of recurrent stroke by about 20% for common stroke. Therefore, although it has not been tested specifically in CADASIL patients, most doctors would recommend that patients with CADASIL who have had stroke take a small dose of aspirin (75- 300mg/day). An alternative to aspirin is clopidogrel (75mg/day). In CADASIL patients who have not suffered a stroke, there is no clear indication for aspirin. We avoid warfarin, or taking the combination of aspirin and clopidogrel, unless required for another medical reason, as this can increase the risk of bleeding within the brain in people with CADASIL.
If required during attacks of migraine, standard migraine painkillers can be taken. These include drugs
such as Migraleve. Initially it was recommended not to take Triptan anti-migraine drugs such as Imigran, but a recent analysis found these were safe in CADASIL and helped migraine attacks in about half of patients.
It is important to look for, and treat when necessary, depression in patients with CADASIL. This can be treated with standard anti-depressant drugs and cognitive behavioural therapy (CBT).
CADASIL2
Most cases of CADASIL are caused by genetic variation in the NOTCH3 gene. However, some cases can be caused by variation in other genes, and the most common of these is HTRA1. This produces a very similar disease with a similar inheritance pattern (autosomal dominant) and similar symptoms of stroke, migraine and cognitive impairment. The MRI appearances are also similar. This disease is often called CADASIL2. We are still finding out about it, as it has only been relatively recently discovered, and there have been far fewer cases described. The data we have so far suggests treating cardiovascular risk factors such as high blood pressure, and stopping smoking and taking regular exercise, is as important as it is for CADASIL. The next section on family testing also applies to CADASIL2.
Should other members of the family be tested for the disease?
For the reasons explained above, if one member of a family has CADASIL, there is a 50/50 chance that close relatives will also be at risk of the disease. If the underlying genetic abnormality is known it is relatively simple to look for it in other family members. This will allow us to be 100% sure whether or not an individual carries the CADASIL gene and is at risk from the disease.
Before testing family members for CADASIL, it is very important that a careful discussion of the pros and cons is carried out. This is usually performed by a genetics counsellor. The knowledge that a healthy person is likely to develop CADASIL can obviously be very distressing, and it is possible that it could influence a number of factors including things such as life insurance. Therefore we would normally only test other family members if they are absolutely certain that this is what they want. It would be extremely unusual for us to test children.
A potential advantage of being tested for the disease is that if you are having children, it is possible to determine whether a foetus carries the disease. If you have the abnormal gene, any children you have also have a 50/50 chance of having the abnormal gene. However, if the abnormal gene has not been passed to you, neither you nor your children are at risk. If a patient with the CADASIL gene (either male of female) is planning to become pregnant it is now possible to have a baby who does not have the CADASIL gene by using pre-implementation genetic diagnosis (PGD). This is a type of in vitro fertilization (IVF) in which embryos in a dish are tested to identify ones that do not have the CADASIL genes, and these embryos are then implanted into the mother.

Cambridge and CADASIL
At Cambridge we have a particular interest in CADASIL. We have a research programme and run a clinical service for patients with CADASIL.
Research Programme
We have an active research programme in CADASIL. If you attend our clinic we may ask you whether you would like to take part in research studies. If you are interested, we will explain the specific details of any individual study and it is always entirely up to you as to whether you take part. Before we plan any study, it is always approved by the local hospital ethics committee. We have a CADASIL research register which we will offer to recruit you to. This allows us to use your clinical, brain imaging and genetic data anonymously to answer questions about CADASIL. We are carrying out projects in CADASIL looking at better ways to treat and diagnose it. Many of these are with our international colleagues throughout the world.
Our research programme has greatly benefited from donations in the past and we are grateful to all our supporters. We welcome donations to our research programme. All donations go into a CADASIL fund which is managed by Cambridge University. Donations can be made to CADASIL Support UK (opens in a new tab) who collect donations for our work, or to the University of Cambridge CADASIL fund via the following online link: Clinical Neurosciences Donation (opens in a new tab). In the box “What prompted your gift today?” please specify ‘Prof Hugh Markus Research, CADASIL fund RREX EFKM’. Do tick the gift aid box if you are eligible, as it increases the amount that goes to our research.
Clinical Service
At Addenbrooke’s Hospital in Cambridge we have a CADASIL clinic at which we see patients suspected of having CADASIL, or family members who wish to have genetic screening. Referrals can be made by your neurologist/stroke physician or your GP to the address at the bottom of this page. We see new patients in person at Cambridge, after this we can see follow-ups by video telemedicine.
Where to find more information on CADASIL
Because CADASIL is a rare disease, and because much of the information on it is very new, it is quite difficult to access accurate information. Some of the information found on the internet is misleading or incorrect. We have set up the CADASIL website (opens in a new tab)
Link: Cadasil.co.uk (opens in a new tab)
to provide a reliable source of information for patients and relatives alike.
On this site there is a wealth of information written in lay language along with links to other helpful websites. It includes information such as:
· Information on all aspects of CADASIL
· Videos on the disease, including clinical management, psychological management of psychological and cognitive problems, patient stories, and research advances
- Recordings from our annual CADASIL meetings
- Frequently asked questions
- News about our regular patient and family meetings which are open to all worldwide
- News on research advances
We would also recommend a UK patient and family CADASIL support group with whom we work closely: CADASIL Support UK (opens in a new tab)
. This is a good way to make contact with other CADASIL families and obtain practical advice on CADASIL.
Professor Hugh Markus
University of Cambridge
Department of Clinical Neurosciences
R3, Box 83
Cambridge Biomedical Campus
Cambridge CB2 0QQ
United Kingdom
Updated July 2025.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/