Introduction
This leaflet has been written to provide information to parents and families whose baby has been diagnosed with an intra-abdominal cyst and aims to support the discussion you have had with your baby’s consultant and care team.
What are intra-abdominal cysts?
Intra-abdominal cysts are fluid-filled growths found in your baby’s abdomen which would not normally be found there.
There are a variety of causes for abdominal cysts. some possible causes are as follows:
Type 1 duodenal atresia: This is a partial blockage of the first part of your baby's small intestine which would require a bypass surgery in the first week of life to allow them to establish feeds. The long-term outcome is very good in the majority of cases.
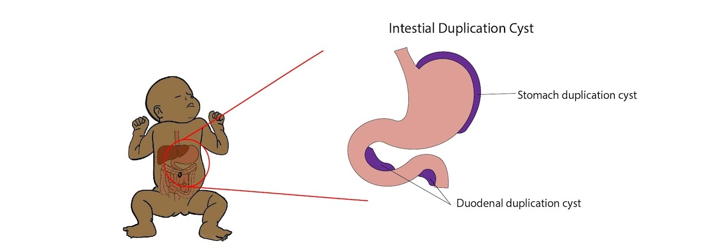
Duodenal duplication cyst: A section of the baby's intestine forms a duplicate part which can cause a compressive blockage to the affected bowel, get infected or have a bleed into it. Therefore, this would need corrective surgery. If the duplication cyst involves bile or pancreatic ducts, this would be done in a liver centre.
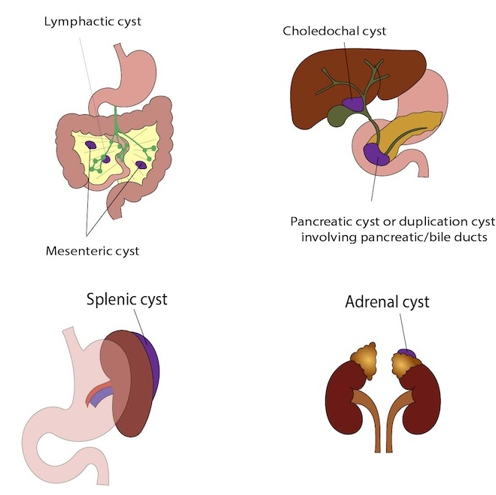
Choledochal cyst: The MRI comments on a normal gallbladder but has not excluded a choledochal cyst. Choledochal cysts result from an abnormal development of the bile duct from the liver to the gut and can lead to problems such as jaundice, infection, pancreatitis and liver failure. This would also require surgery in a hospital with a specialist liver team.
Pancreatic cyst: This is a rare condition in which there is a cyst in the pancreas. Children with this type of cyst would be referred to a hospital with a specialist liver team.
Splenic cyst: This is a cyst which occurs in the spleen. Splenic cysts require monitoring but usually no surgery.
Adrenal cyst: The most likely management of cysts in the adrenal glands is monitoring and blood tests of adrenal hormones. Interventions are only needed if the baby is symptomatic.
Mesenteric cyst: This is a cyst within the fatty support tissue that carries the blood supply to the bowel for which occasionally a simple excision is indicated if the cyst is large.
Lymphatic cyst: A cyst within the lymphatic system in the abdomen; often the management is conservative but occasionally intervention is offered.
Some possible locations of intestinal duplication cysts are shown in the diagram below:
Diagrams showing other types of cysts which your child may be diagnosed with after birth:
What causes abdominal cysts?
Most foetal abdominal cysts develop due to an unexpected interruption in the normal growth process which creates an additional layer or fluid-filled sac. The exact cause remains unknown, and there is nothing the baby's parents can do to prevent the formation of these cysts.
Signs and symptoms
The cysts typically don't cause any symptoms during pregnancy. In some cases, doctors can detect the cyst in the baby's abdomen after birth. Other signs of a foetal abdominal cyst after birth may include:
- difficulty feeding
- crying and fussiness due to pain
- yellowing of the skin and eyes (jaundice)
- vomiting
- difficulty with bowel movements
- difficulty urinating
What happens after birth?
We will need to keep an open mind and consider many possibilities. There still remains diagnostic uncertainty and we need to evaluate the baby postnatally, both clinically and with further medical imaging (scans), to be able to better understand the nature of this cyst.
Treatment and Management
The priority will be to ensure your baby is able to tolerate feeds prior to discharge and we will take a stepwise diagnostic approach.
If the delivery is uncomplicated and your baby is well, your baby can stay with you for some skin-to-skin time and a small nuzzle at the breast. Your baby will then need to be admitted to the neonatal unit, where your baby will be assessed by the team, as well as the surgical team. We would not feed your baby until we know that there is no blockage and insert a tube via the nose into the stomach (called a nasogastric tube) to decompress the stomach. Your baby can have colostrum for mouth care, but a drip will be inserted to provide fluid and glucose.
Investigations
Baseline blood tests: These will be done for your baby after birth.
Abdominal x-ray: These will be done no sooner than 8 hours of age, to assess for a bowel blockage (called ‘double bubble’). Your baby may also require a contrast study (contrast is a fluid which shows up on x ray) to help identify specific causes of blockage such as a type 1 duodenal atresia (see description above) or obstructing duplication cyst (see description above). In case there is a blockage, your baby would need corrective surgery prior to discharge, so that feeding can be established. This may require a hospital stay of a few weeks.
Abdominal ultrasound scan: If no blockage is found we will request an abdominal ultrasound scan as an inpatient. It is possible that once the baby is fully fed your baby can be discharged for further outpatient imaging and surgical follow up scans as an outpatient as directed by the ultrasound findings.
MRI scan (MRCP): The aim is to identify the underlying cause of the cyst and prevent complications in the future by arranging monitoring and timely surgery as required, either at Addenbrooke's Hospital or in a specialist liver centre, likely to be Kings College Hospital in London.
More information about the neonatal unit
Being apart from your baby will be difficult and we will show you how to have positive touch experiences from the start even if a cuddle might not be possible right away. Parents are allowed to visit at all times, but there is limited accommodation available for parents of babies in the Neonatal Unit. We try to provide accommodation around the time of admission, surgery and in preparation for discharge home. If you would like to visit the Rosie neonatal unit prior to delivery, please ask the foetal medicine team to contact Neonatal Intensive Care Unit (NICU) to arrange this. A short video introducing the NICU is also available in the Neonatal Services section on the Rosie Hospital website.
Support for you and your child with abdominal cyst
ERIC is the national charity dedicated to improving children’s bowel and bladder health. Their mission is to reduce the impact of continence problems on children and their families. Click here for the Eric website. (opens in a new tab)
BLISS provides support, advice and information for the parents and families of babies born prematurely, requiring intensive care and/or special care. Also works with bereaved families. Click here for the Bliss Website (opens in a new tab).
Chaperoning
During your child’s hospital visits your baby will need to be examined to help diagnose and to plan care.
Examination, which may take place before, during and after treatment, is performed by trained members of staff and will always be explained to you beforehand. A chaperone is a separate member of staff who is present during the examination.
The role of the chaperone is to provide practical assistance with the examination and to provide support to the child, family member/ carer and to the person examining.
Contacts/Further Information
Office: 01223 586973
(Mon to Fri 08:00 to 18:00 except bank holidays)
Illustrations in leaflet kindly produced by Imogen Seago.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/