Your surgery
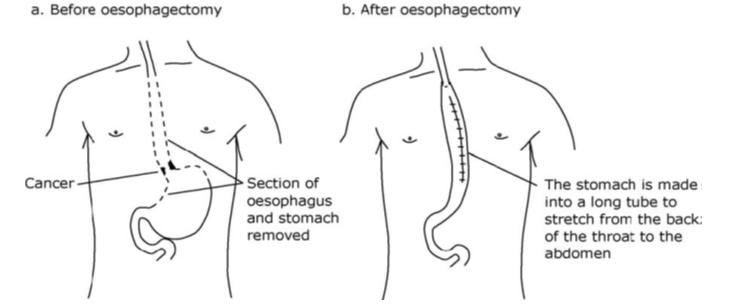
The role of the oesophagus is to transport food from your mouth to your stomach. During your surgery most of your oesophagus is removed; the stomach is moved into the chest becoming a tube-like shape. It is then re-joined to the remainder of the oesophagus. Depending on where the tumour was located it may also have been necessary to remove part of your stomach.
The diagram below shows what you what your stomach looks like before and after an oesophagectomy.
The surgery will affect the way that you eat as the stomach can no longer stretch to accommodate large portions of food. It can take a number of months to recover and adjust to eating and drinking after surgery, however it is important that you receive enough nutrition in order to help fight infections, heal surgical wounds and support your recovery. It is also essential that you do not lose too much weight. Hence, we support your recovery initially with a feeding tube.
Enteral Tube Feeding:
As part of your operation you will have a feeding tube placed into part of your small intestines (the jejunum). This is called a jejunostomy feeding tube (jej tube). You will be seen by the Dietitian on the first day after your operation; they will prescribe a nutritionally complete liquid feed that is given via the feeding tube. Your oral intake will be limited to small amounts of water or clear fluids for the first 5-6 days following surgery. All your nutrition at this time will be provided through the feeding tube, delivered at a steady rate over 24 hours via a pump.
Oral intake:
Your oral intake will progress from water to clear fluids (fruit squash, black tea/ coffee, Bovril, jelly or clear soups); to free fluids (milky drinks, hot chocolate, ovaltine, ice cream, smooth yoghurt, soups without lumps); to puree diet (see section on Diet One) whilst you are in hospital.
Your tube feed will be changed to overnight as you start to eat. When you go home, your nutritional needs will be met with a combination of both tube feeds and puree diet.
The length of time you require a tube feed will depend on how well you are able to progress with your eating. This can range from as little as 4 weeks to approximately 15 weeks and can depend on whether you also have further treatment after surgery. Your Dietitian will reduce your feed in stages, as the amount you are able to eat increases, before the tube is removed.
See separate information on looking after your feeding tube and your feeding plan for home.
Key tips for once you start eating and drinking:
- You will need to take food little and often, for example 6 small meals per day. This is a lifelong change that will need to be followed after your surgery to ensure you take in adequate nutrition over the duration of the day.
- Aim to keep all portions equal in size. Palm size or small cup size.
- Drinking is important; however avoid drinking large volumes with food. Leave approximately 30 minutes before or after eating. It can be difficult to drink enough therefore aim to keep drinking small amounts in between meals.
- Take time over your meals and chew foods well.
- Avoid eating large amounts close to bedtime as this can increase your risk of reflux.
- Focus on high calorie and nutritious foods and drinks.
- Fortify your meals by adding extra calories from butter, margarine, oils, whole milk, cream, cheese, pesto, ground nuts, crème fraiche or coconut cream.
- Nutritional supplement drinks (e.g. Fortisip, Fortijuce, Fresubin drinks) are generally not recommended following your surgery as they can cause ‘dumping’ symptoms.
Diet One: Puree (IDSSI Level 4) + Melt in the Mouth Foods
Once the team are you happy that you are tolerating free fluids you will be started on pureed foods. You should follow this diet for approximately 14 days Foods should be smooth and moist with no solid lumps.
- Use a hand blender or food processor to puree foods. Cook all food until tender and cut into small pieces before liquidising.
- Additional liquids or sauces such as full fat milk, coconut milk, stock, gravy and cream should be used to create the desired consistency (and add calories).
- Puree foods can look more appetising if they are presented separately (e.g. liquidising a meat casserole and vegetables separately to serve.)
- Remove tough skins and large seeds before blending.
Keep portion sizes to small and frequent. It is suggested that portion sizes for ‘meals’ and ‘snacks’ are limited to about a hands palm size, or small cup or bowl. These should be consumed 6 times per day.
Do not worry if your portion sizes seem much smaller to start; your tube feed via your jejunostomy will be tailored around your diet to make sure your nutritional needs are fully met.
Meal suggestions: Diet One
Aim to eat six small meals/ snacks per day
Breakfast ideas:
- Smooth porridge or Ready Brek made with whole milk
- Weetabix soaked in milk
- Full fat yoghurt or fromage frais (add fruit such as well mashed banana, stewed fruit or fruit puree)
- Pureed scrambled egg
- Homemade milkshake or yoghurt drink
Main meals:
Meat, fish and alternatives
- Puree meats by adding gravy, tomato sauces, creamy sauces or creamy soups. You can add extra sauces such as cranberry, mint, apple, soy for flavour.
- Puree fish with white sauce, parsley sauce, cheese sauce, hollandaise sauce or tartar sauce.
- Fish mousse or light pate.
- Pureed scrambled eggs with added cheese.
- Pulses (e.g. chickpeas, butter beans) can be pureed with olive oil and flavourings to make houmous or dips.
- Puree beans or lentils added to tomato sauces, soups or curries (e.g. dhal.)
Starchy foods and vegetables:
- Smooth soups: these can be homemade, tinned or fresh (fortify with extra cream, milk powder, ground nuts, pesto or coconut milk.)
- Potatoes, sweet potatoes or butternut squash can be cooked and mashed with cheese, butter and/ or whole milk.
- Puree or mash cooked vegetables with butter, a sauce or a little extra liquid (root vegetables often mash the best.)
- Puree vegetables such as cauliflower, broccoli, mushrooms or leeks with a cheese or creamy sauce.
Snack and dessert ideas:
- Full fat yoghurt, mousse or fromage frais.
- Pureed or ground rice pudding, semolina, milk jelly, crème caramel, Angel Delight.
- Stewed fruit or mashed banana with custard or ice cream.
- Biscuits dunked in a warm milky drink.
- Bowl of cereal (e.g. Weetabix, Shreddies soaked in plenty of soup or Ready Brek.)
- Mashed avocado or guacamole.
- Corn snacks or light crackers that ‘melt in the mouth’ (e.g. Cheddars, Tuc or Ritz biscuits, Wotsits, Skips or Quavers) with dips (e.g. houmous, taramasalata, tzatziki.)
Nourishing drinks:
- Cold milk, milkshakes, iced lattes/ frappes (add milk powder and/ or ice cream)
- Hot milky drinks (e.g. latte, hot chocolate, malted drinks)
- Smoothie (liquidise fruits with whole milk and yoghurt)
- Enriched soups (e.g. Complan Soup or Meritene Soup)
Diet Two: Any foods within the following textures: Level 5 (minced and moist), Level 6 (soft and bite size) and Level 7 (‘Easy Chew’ selections)
After 14 days of eating a puree diet you will be able to increase the texture of the foods you are having. You should follow this diet for 4 weeks.
- Soften foods by chopping, mincing or mashing
- Use lots of sauce, gravy, butter, cream or custard to soften and moisten foods
- Make sure vegetables are well cooked and meat and fish are cooked until tender
- Avoid foods that require lots of chewing, stringy foods, tough skins or crispy coatings
- Foods from diet one can be used however vary with the texture options of foods from the list below as well
Meal suggestions: Diet Two
Continue to eat little and often – six small meals/ snacks per day
Breakfast ideas:
- Porridge or Ready Brek
- Cereal soaked in lots of milk (e.g. Rice Crisipies, Cornflakes, Weetabix)
- Scrambled egg or an omelette (add cheese or smoked salmon)
- Baked beans
- Tinned or stewed fruit with full fat yoghurt or fromage frais
- Toast if softened with baked beans or scrambled egg (remove bread crusts)
Main meals:
Meat, fish and alternatives
- Shepherd’s pie, cottage pie, corned beef hash
- Minced meat with gravy or sauce (e.g. bolognaise)
- Tender stews, hotpots, casseroles or moussaka
- Potted meat or pâtés
- Fish in a white, parsley or cheese sauce (e.g. fish pie or fish mornay)
- Tinned in fish with a sauce (e.g. mayonnaise, tomato, olive oil)
- Egg mayonnaise, scrambled egg or omelette with cheese
- Baked beans
Starchy foods and vegetables:
- Mashed, boiled or baked potatoes (without the skins)
- Pasta in a sauce (e.g. carbonara, macaroni cheese, ravioli)
- Spaghetti hoops
- Cauliflower cheese
- Soft vegetables that could be mashed with a fork, mashed or easy chew vegetables
- Ratatouille
- Soups with small pieces of vegetable, potato, pasta or pulses
Snack and dessert ideas:
- Milk puddings, e.g. rice pudding
- Sponge and custard, fruit crumble and custard
- Trifle
- Pancakes with a sauce or ice cream
- Crackers/ bread sticks with soft cheese, dips, houmous or pate
Include nourishing drinks in between meals and snacks.
Diet three: Normal Diet
After about four weeks on Diet Two textures you should be able to manage most foods. Although the portion sizes you can manage may be larger than when you first started eating and drinking you should still keep to a little and often eating pattern to meet your nutritional needs and avoid problems associated with eating larger portion sizes.
It is important to try to eat a balanced diet that includes:
Starchy Foods (carbohydrates):
Include one of the following at each meal: bread, breakfast cereals, pasta, rice, potatoes, noodles, crackers, crisp bread, couscous, bulgur wheat, quinoa.
Protein foods; meat, fish and alternatives:
Aim for two portions per day; meat, poultry, fish, eggs, lentils, beans, nuts, tofu, quorn, soya.
Milk and Dairy products:
Dairy products are good sources of calcium, protein and energy. They include milk, cheese, quark, yoghurts, fromage frais and rice/ nut/ soya milk and yoghurt alternatives. Aim for two or three portions a day.
Fruit and vegetables:
Aim for five portions of fruit and vegetables every day. Fresh, frozen or tinned all count.
Fatty and Sugary foods:
Mayonnaise, butter, oil, cream and cheese can be added to many foods to provide more energy.
Sweets, chocolates, fizzy drinks and high volumes of juice drinks can pass through your stomach quickly and may cause diarrhoea and cramping – “dumping syndrome”
Vitamin Supplements:
Due to the surgery it can be difficult for your body to process and absorb all the vitamins and minerals it needs from diet alone. We would therefore recommend taking a daily complete multivitamin and mineral supplement. Look out for ‘A-Z’ multivitamin and mineral supplements as these will be complete in both the minerals and vitamins that you require. They can be purchased from most supermarkets or pharmacies. Some supermarkets also have a chewable ‘A-Z’ which you may find helpful if you have trouble swallowing tablets.
Difficulties you may experience following your Oesophagectomy
An oesophagectomy significantly changes your digestive tract and can cause short and long term changes to your eating. If you are experiencing any symptoms you are concerned about discuss them with the team.
Swallowing
After surgery, scar tissue can form at the surgical join in your oesophagus. This may restrict your ability to swallow solid food or feel like a lump in your throat. This can often be treated by dilating (stretching) the join during an endoscopy. It is a routine procedure but may need to be repeated a few times in the early months. Do not allow the problem to persist for too long, contact your specialist nurse to arrange an endoscopy and your dietitian for dietary advice.
Dumping Syndrome
Dumping syndrome is a group of signs and symptoms that can occur after an oesophagectomy. The altered digestive system affects the rate that food passes through, i.e. it may pass through more quickly, causing a number of possible symptoms. These can include, bloating, nausea, palpitations, flushing, sweating, faintness, tiredness, loose stools or diarrhoea.
The signs and symptoms of dumping are often experienced soon after a meal (within 15 to 30 minutes). However they may occur later (one to three hours after eating). They are therefore often referred to as ‘early’ and ‘late’ dumping syndrome.
Not everyone will experience dumping syndrome. For those who do, symptoms may be unpleasant and distressing initially, however by following simple dietary measures and learning how to manage symptoms people often find episodes become less problematic or less frequent over time.
Dietary measures include:
- Eating small, frequent meals every 2-3 hours
- Eating slowly and chewing foods thoroughly
- Limiting fluid consumption during meals. Drink liquids at least 30-60 minutes before or after meals instead of with meals.
- Avoiding foods and drinks that are high in sugars (such as sweets; sugary cakes, sugary breakfast cereals; jams and conserves; sugary fizzy drinks; and nutritional supplement drinks, e.g. Fortisip and Fortijuce).
- Including good sources of protein and/ or fats with meals
- Choosing more foods that are high in soluble fibre (such as pulses, oats, fruits and vegetables)
If you experience any of these symptoms it is important you discuss these with your dietitian for further advice.
Change in Bowel Habit
It is very common to have changes in your bowel function after this surgery. You can experience diarrhoea, constipation or a change in the appearance or colour of your stools. Bowel habits can often be more unsettled in the early stages after surgery and improve over time. However you may also see changes in your bowel habits a number of months after surgery.
It is important to talk to your team about it. Often it can be improved by dietary changes and /or medication.
Loss of Appetite
Most patients who have had an oesophagectomy report loss of appetite and loss of interest in food at some point in their recovery. This can last a few weeks or years. Appetite stimulation is a complex process, but it is partly controlled by the production of hormones produced in the top part of your stomach. As this part may have been removed it is possible you won’t get the same ‘brain messages’ to say you are hungry.
Just because you are not feeling hungry, it doesn’t mean you don’t need the calories from your food. Try to eat by the clock (every 2-3 hours) rather than waiting until you are hungry.
Tips to stimulate your appetite:
- Go for a short walk or get some fresh air before your meal
- Relax and avoid rushing meals
- Try using a smaller plate and serve meals which are attractive and colourful
- If food has no taste, try stronger flavours such as seasoned or marinated foods
- Make the most of the foods that you enjoy
- Avoid drinking large amounts of fluids, particularly before or during a meal, this can leave you feeling full and reduce the capacity for food.
Acid Reflux
Reflux is a common problem after this type of surgery. The symptoms can be a burning feeling or pain in your chest area or throat, an unpleasant taste, nausea or coughing. Symptoms may be more predominant at night or on waking. Reflux can be treated by taking an acid suppressant (e.g. lansoprazole or omeprazole). You should liaise with your specialist nurse or GP regarding the dosage and timing of your medication.
You should avoid lying flat when sleeping after this type of surgery. Using extra pillows or raising the bed head by placing blocks under the legs at the head of the bed is often beneficial. If you are experiencing any of these symptoms at night, try to avoid eating too late in the evening. Aim to have your last meal or snack 2-3 hours before going to bed.
Chyle leak
Chyle is a milky liquid formed by the body after eating food or drink containing fat. Chyle is transported around the body in the lymphatic system (a network of thin tubes/ vessels that run throughout your body).
What is a chyle leak?
During an operation the vessels in the lymphatic system can be damaged and the chyle can leak out. This may be collected in one of your drains; it often appears as a milky fluid. In this instance the surgeons may suggest following a low fat diet/ enteral feed in an attempt to produce less chyle and aid healing. If this is the case your Dietitian will give you more information and support on doing this.
Information and Support
This leaflet is intended to give you basic information following your operation. If you have any questions or anxieties, do not hesitate to discuss them with your dietitian, clinical nurse specialist, or doctor.
Specialist Upper GI oncology dietitians: 01223 216655
Upper GI clinical specialist nurses: 01223 596383
Nutrition nurse specialists: 01223 216037
Contacts
The Oesophageal Patients Association
The Oesophageal Patients Association was founded to provide support and reassurance to patients with oesophageal disease. All members are patients, and many have had an oesophageal tube inserted. Contact details are outlined below:
Oesophageal Patients Association
Registered Office 22 Vulcan House,
Vulcan Road,
Solihull,
West Midlands
B91 2JY
Chairman: Professor Robert Mason | Registered Charity No. 1062461
Telephone: 0121 407 9860 (09.00am – 15.00 Monday – Friday)
Answerphone for out of hours callers
Website: www.opa.org.uk Email: opa@ukgateway.net
Macmillan Cancer Support
Macmillan Cancer Support (opens in a new tab)
Call us free * on 0808 808 00 00 (Monday to Friday, 9am–8pm)
Lily UK, videos
Privacy & dignity
Same sex bays and bathrooms are offered in all wards except critical care and theatre recovery areas where the use of high-tech equipment and/or specialist one to one care is required.
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/