The operation that you have had has successfully removed your endometrial (womb) cancer. However, there may be a few undetectable cancer cells which can cause the cancer to return at a later date. Having radiotherapy treatment at this stage may reduce the chance of the cancer returning.
This leaflet explains the benefits, risks and alternatives to undergoing radiotherapy following your surgery. We want you to be informed about your choices to help you be fully involved in making decisions about your treatment.
Please ask about anything you do not understand or wish to have explained in more detail.
About Adjuvant Radiotherapy
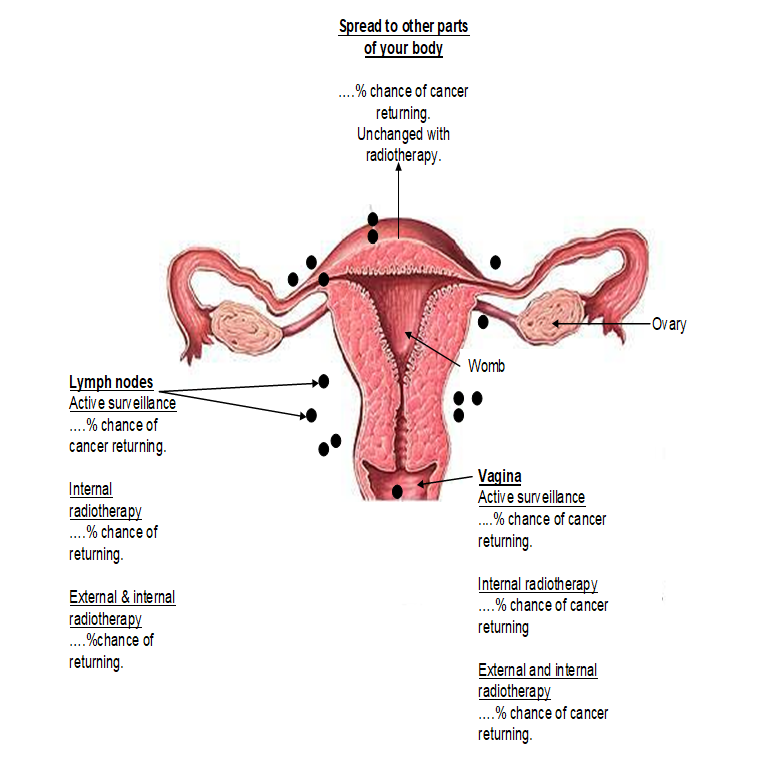
The operation that you have had has completely removed your cancer. With no further treatment your chance of being cured (the cancer never returning) is around ………%. On the next page is a diagram showing you the areas where the cancer may return and the how the different treatment options may affect the chance of the cancer returning.
Current evidence suggests that radiotherapy for cancer of the womb decreases the risk of local recurrence but does not improve survival.
Your choice of treatment
It is often difficult to make a decision about which treatment option you should have. It is important that you discuss any concerns you have regarding your decision with your doctor or radiographer. The table below summarises the benefits and risks of each treatment to help you make a decision.
| Active surveillance |
Brachytherapy (internal radiotherapy) |
External and Internal radiotherapy | |
| Process |
Follow up will be with the surgical team responsible for your operation. The follow up schedule will be determined in conjunction with your surgeon |
One outpatient treatment a week for three weeks. Vaginal applicator inserted for 10 minutes. Treatment painless Follow up schedule: Three monthly for one year then six monthly for two years. |
CT planning scan Three tattoos 25 outpatient treatments, every day (Mon-Fri) for five weeks. This may or may not be followed by one internal treatment. Follow-up schedule: Appointments at 3 months, 9 months and eighteen months |
| Benefits |
No side effects Radiotherapy is only given if your cancer returns in the pelvis. At least 50% chance of cure if radiotherapy is given at this point. |
Risk of vaginal recurrence reduced to less than 5% No significant side effects |
Risk of vaginal and pelvic recurrence reduced to less than 5 % |
| Risks |
Cancer may come back in your pelvis or vagina. This might have been prevented with early radiotherapy. Cancer may come back somewhere else in your body. No improvement in survival. |
Vaginal stenosis (shortening and narrowing of the vagina) - this may be prevented with regular use of vaginal dilators Cancer may still come back in your vagina despite radiotherapy. Cancer may come back in your pelvic lymph nodes that may have been prevented with external radiotherapy. Cancer may come back somewhere else in your body. No improvement in survival. |
Significant risk of side effects: Acute (during treatment and up to six weeks after treatment completed) Diarrhoea Cystitis - frequency, urgency, pain Abdominal (tummy) cramps Skin reaction (in area being treated) Fatigue Long term (six months to many years after treatment completed) Bowel change - diarrhoea, urgency, abdominal pain, incontinence Recurrent cystitis Bleeding from the bowel or bladder Vaginal stenosis Pelvic bone pain 5-10% chance of permanent serious bowel or bladder side effects that may require you to have an operation. Cancer may come back in the pelvis or vagina despite radiotherapy. Cancer may come back somewhere else in your body. No improvement in survival. |
We are smoke-free
Smoking is not allowed anywhere on the hospital campus. For advice and support in quitting, contact your GP or the free NHS stop smoking helpline on 0800 169 0 169.
Other formats
Help accessing this information in other formats is available. To find out more about the services we provide, please visit our patient information help page (see link below) or telephone 01223 256998. www.cuh.nhs.uk/contact-us/accessible-information/
Contact us
Cambridge University Hospitals
NHS Foundation Trust
Hills Road, Cambridge
CB2 0QQ
Telephone +44 (0)1223 245151
https://www.cuh.nhs.uk/contact-us/contact-enquiries/